Emergency Medical Services - 1939-1945
‘A few years ago when a very distinguished personage, as president of a great teaching hospital, was inaugurating the first installment of a rebuilding scheme, he pressed a button and started a light revolving on the top of the tower. Taken a little aback, he turned to the Dean who was standing by him and murmured: “Good Lord, what have I done now?” We can imagine the Minister of Health making some such ejaculation when he first realised the inexorable upshot of his Emergency Hospital Scheme. Designed to serve the purpose of a moment it has set going wheels which will turn and turn until the whole aspect of hospital and consulting practice, as we knew them as lately as the end of last August, has changed beyond recognition.’ The Lancet’ After Sir Charles Wilson’s committee had reported on how London’s hospital service might be organised to meet the threat of bombing, the London County Council seconded staff to the Ministry to assist the subsequent planning of medical and ambulance services. In October 1938 negotiations started with the voluntary hospitals to establish a segmental scheme but progress was slow. Sir Frederick Menzies contrasted the efficiency with which the municipal hospitals could be organised with the difficulties experienced ‘in bringing about a willing cooperation on the part of the voluntary hospitals’. The Minister of Health, Mr Walter Elliot, was told by his officials that Sir Frederick rather exaggerated the contrast between the rectitude of the LCC and the depravity of the voluntary hospitals, although some of the hospital representatives had not been so helpful as they might have been.2 One of the sticking points was who would command the sectors. The creation of the emergency medical service
It was thus the threat of the Luftwaffe which compelled Britain — and
London — to reorganise the hospital services. Many detailed and
practical problems had to be sorted out and the London Voluntary
Hospitals Committee became increasingly anxious that while the
Ministry’s scheme was all right as far as it went, few staff had been
allocated to the task; they had inadequate authority and virtually no
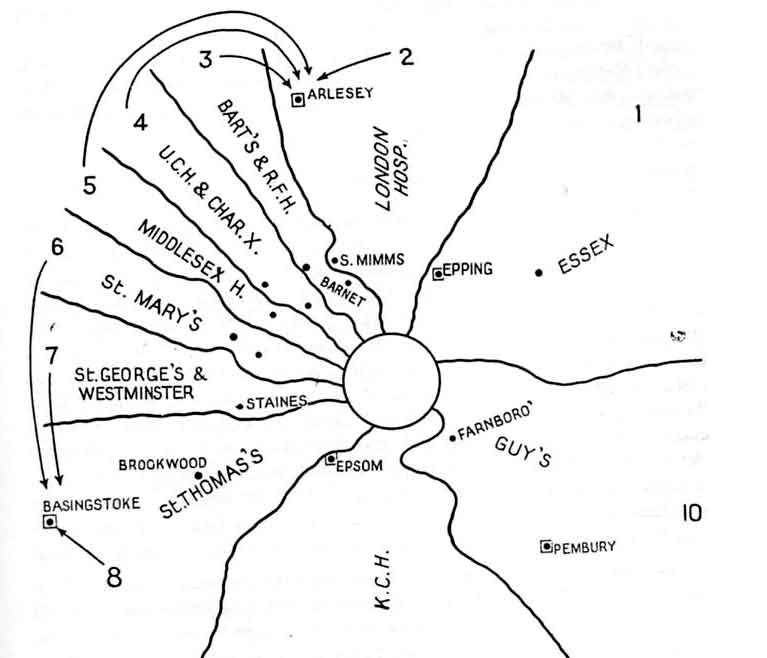
money The committee made a series of proposals which it wished to see laid before the Minister and, if necessary, the Cabinet. Adverse comments appeared in the press which Sir Charles Wilson disavowed. The Minister took a month to reply, and rejected the suggestion of failure to take the situation seriously. Nevertheless, senior members of the teaching hospitals’ staff were soon appointed as the first medical sector officers, and in June 1939 house governors and matrons were nominated as lay sector officers and matrons. Financial arrangements were also made for the establishment of first-aid posts and the sandbagging of the hospitals.3 The Metropolitan Police District and the area within about forty miles of it was divided into ten sectors. The general aim was to establish first-aid and casualty sorting centres in the danger areas, providing enough treatment to fit casualties for a journey by ambulance to advance base hospitals. These were in presumably safer areas, with enough staff and equipment for operative treatment of the injured. Base hospitals to which patients could be moved for after-care were still further from the centre. Finally there was a group of less well equipped hospitals for convalescent and chronic cases. The sector officers began the task of surveying the strange assortment of mental asylums, public assistance institutions and other hospitals which were at their disposal. They considered plans for the evacuation of staff and students.4 Contact was established with Sir Frederick Menzies and other medical officers of health, and a map was published in The Lancet showing the arrangement of the sectors and the position of the advance base hospitals.5 Nine sectors radiated from an apex in the centre of London into the home counties, and were based on one or more of the teaching hospitals; the Essex sector was based upon hospitals in Stratford, Ilford and Romford (see Table 20, page 240, and Figure 12, page 241). At their extremities the sectors included parts of Essex, Hertfordshire, Buckinghamshire, Kent, Surrey and Berkshire which strictly belonged to other home defense regions — the regional organisational pattern established for military purposes. The London sectors
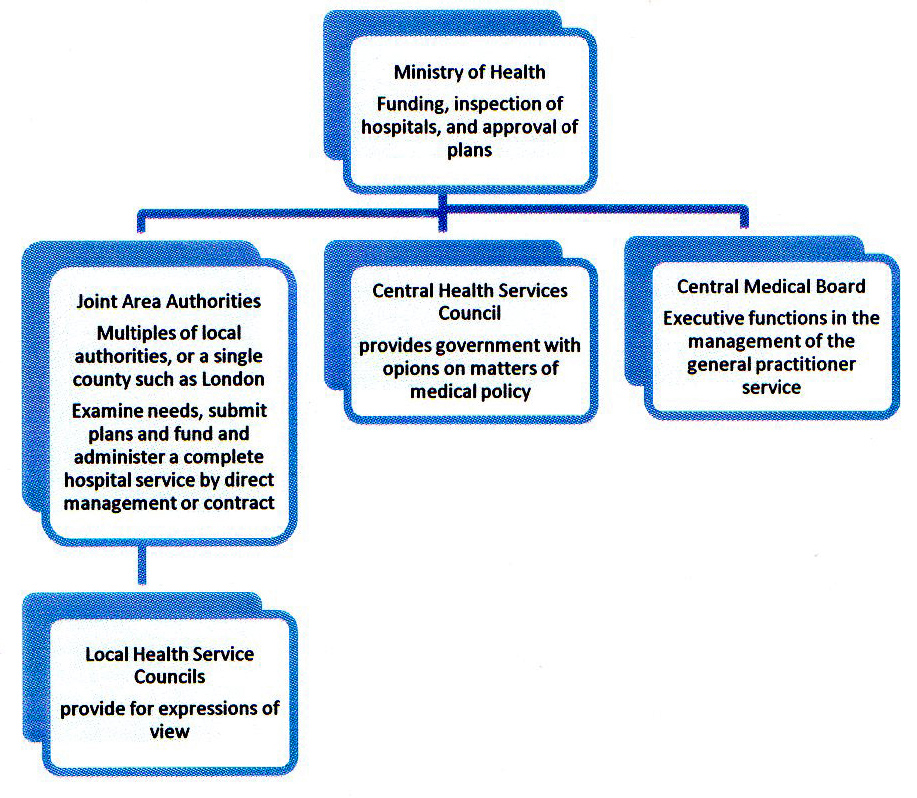
Map of London Sectors Source: The Lancet 1939, i, p723 The Emergency Medical Service was introduced as soon as war broke out, and gave central government a right of direction over both voluntary and municipal hospitals which it had never before possessed. Patients were discharged or evacuated from the hospitals in central London in preparation for a wave of air-raid casualties which did not materialise. The staff who had been evacuated had little to do. Some occupied themselves treating local patients, many of whom had never previously had the benefit of specialist attention. Meanwhile, hospital beds stood empty in central London until, at length, limited services were resumed. In spite of the casualties which followed the evacuation from Dunkirk and the London blitz of 1940—1941 the Emergency Medical Service was never placed under the stress which had been predicted and for which it had been designed, serious though the damage from bombing proved to be. However the Emergency Medical Service, more than any other single factor, can be held responsible for the form and pattern of hospital organisation which emerged in London. A certain amount of friction existed between the two parts of the system, based on traditional insularities of outlook, but not so much as to prevent a synthesis of the two groups of hospitals. Doctors and nurses for the first time moved freely between the voluntary and the municipal hospitals, seeing the problems each faced. The experiences of teaching hospital staff and students who were drafted to municipal hospitals, where standards of clinical care often left much to be desired, helped later in the acceptance of the National Health Service. The senior officer in each sector had direct access to the Permanent Secretary at the Ministry of Health, and through municipal medical officers at sector headquarters, to municipal hospitals. His main power was the distribution of medical staff to hospitals according to their specialties and skills. The municipal and mental hospitals to be upgraded for casualty purposes had been chosen by the Ministry, largely without the advice of the sector officer. Many hoped that the cooperation which had been enforced through war could be preserved in peacetime. ‘The outstanding merit of the Emergency Medical Service’ said Political and Economic Planning, ‘is that it has begun a process which total war makes absolutely imperative - a pooling and reasonable distribution of medical resources and scientific skill.’ Regrettably, the publication continued, the sectors worked too much as independent units, a situation encouraged by the appointment of distinguished teaching hospital consultants as group officers.6 The group officers, and their administrative counterparts, saw less need than Political and Economic Planning for cross-sector coordination, as most problems could be resolved within the boundaries of their own areas. Within these sectors, links between hospitals were established which persist to this day. The effects of evacuation, fire and bombing are described in hospital histories like Cameron’s account of Guy’s and Clark-Kennedy’s of The London.4 Not one of the London County Council’s hospitals escaped damage. The Poet Laureate, John Masefield, considered writing a history of London’s hospitals under fire, and he obtained a special allocation of petrol coupons to enable him to visit them. Sadly, the project was abandoned. The medical schools, like the hospitals, faced many problems as a result of inadequate accommodation and makeshift laboratories, but in one way or another they were overcome.7 The experience of coping with dispersed students and staff, and trying to teach under such conditions, convinced most deans that decentralised schools were to be avoided. When, after the war, the medical schools were expanded, this conviction led to the demand for large university hospitals. Planning a future hospital service The twists of the negotiations and the complex issues which had to be decided before the introduction of the National Health Service by Bevan in 1948 form a story which has been told elsewhere.8 Lord Dawson’s interim report of 1920 had indicated the hierarchical structure a health service might take. It was followed in the thirties by proposals and reports from several organisations, including the British Medical Association.9 The Nuffield Provincial Hospitals Trust was pressing ahead with the concept of regionalisation, while Wilson Jameson, dean of the London School of Hygiene and Tropical Medicine, organised a Saturday morning group with brought together doctors from many different fields. Known as the ‘Gasbag Committee’, it examined a number of problems including the financial plight of the teaching hospitals. Only the state could provide the large sums necessary but how, asked the group, could the teaching hospitals preserve their much valued independence in such a situation? [There were ten to twelve members of the Gasbag Committee, including Wilson Jameson, until he moved to the Ministry as chief medical officer: W W C Topley, Allen Daley (MOH LCC), H M C Macaulay (MOH Middlesex), George Picketing (St Mary’s), Ernest Rock-Carling, Landsborough Thomson and Harold Himsworth. There was a free exchange of views and notes were not kept as a matter of policy. An attempt was made to gain consensus on major matters of policy and the group met regularly from September 1939 until the Saturday before Dunkirk, August 1940.] Since February 1938 the Ministry had been exploring various options and in October 1939 Sir Edward Forber, who had recently retired from the Board of the Inland Revenue but had been a Deputy Secretary at the Ministry of Health, was invited to enquire into wartime/postwar hospital problems. At the same time The Lancet published a ‘Plan for British Hospitals’ which advocated regionalisation and centralisation, and made biting comments about the London hospitals. The author was Stephen Taylor, later Lord Taylor, and a lengthy and emotive correspondence followed which was summarised in the journal in a statesmanlike fashion by Lord Horder. Picture Post also discussed hospital planning in a special issue on Britain in the future. The authors advocated a salaried state health service which placed an emphasis on preventive rather than curative medicine.10 By 1941 several factors were making it increasingly urgent to establish a postwar hospital policy. The Emergency Medical Service had created the opportunity; a long-term policy was required to decide which hospitals in an area should be preserved and developed; and new and lively bodies like the Nuffield Trust were emerging in the policy-making field. From January to September 1941 a Ministry committee on postwar hospital policy was at work, which had a preliminary paper laid before it containing proposals remarkably like those which ultimately formed the basis of the NHS Act (1946). The committee soon accepted that some form of regionalisation was necessary, because modern health services could not be provided within small local authority areas. Regional authorities could plan services which might then be funded from exchequer funds, insurance contributions and a precept on local authorities. It was recognised that a centrally directed regional organisation would be opposed by local government, and a key question would be the relationship between Whitehall and local authorities. Possibly each area might have a body consisting of local authority., voluntary hospital and medical representatives, the ownership of the hospitals remaining unchanged. It was soon clear that the arrangements which might suit the rest of the country would be inappropriate in London, and that the financial framework would be of crucial importance, particularly to the teaching hospitals. The Office Committee on Postwar Hospital Policy thought that it might be possible to treat the teaching hospitals separately, leaving them a much higher degree of independence. Related to this, in London, was the necessity of maintaining as many as twelve teaching hospitals. The government had been asked to assist the teaching hospitals but Sir Edward Forber, whilst recognising that this was a controversial matter, questioned the need for twelve as some were really too small.11 A paper prepared by John Pater for the committee drew attention to the fact that London contained not only the largest municipal hospital service in the world but ‘a quite disproportionate number of the large voluntary teaching hospitals’ crowded into the centre of the metropolitan area. He suggested two ‘desirable developments’: i. The grouping of hospitals to serve not only the Metropolitan area but also a large part of the home counties. He suggested wedge-shaped areas with their apex in the centre like the Emergency Hospital Scheme sectors. ii. The decentralisation of teaching work. If regional organisation was to be complete, provincial hospitals would have to be developed. The destruction of teaching hospitals by the blitz had created an opportunity for development on rational lines which would be lost if hospitals compelled to leave by bombing were allowed to return and rebuild in the centre of the city. Future plans and the London County Council Whilst this preliminary work was proceeding within the Ministry, and confidential discussions were taking place, the issue of the future hospital service and how it might be organised was raised in a most abrasive fashion by the Leader of the Labour controlled London County Council. It was known that the Nuffield Provincial Hospitals Trust was about to publish a memorandum on regionalisation, and writing in the Star on 12 August 1941, Alderman Latham said: ‘The fifth-columnists against democracy are preparing to steal the people’s municipal hospitals.., the beavers of reaction are ceaselessly gnawing at the foundations of popularly elected local government.’ Latham feared that although three-quarters of London’s hospital beds were provided by the council, to ‘save’ the voluntary hospitals all would be-taken over and handed to non-elected regional bodies, which would preserve the features of the voluntary system but sacrifice public accountability. Instead, he wished to see a comprehensive service administered by the local authorities into which the voluntary hospitals would have to come if they wished to play their part. He warned his readers to be on their guard - ‘sappers against democracy would get them if they did not watch out’. Public disagreements of this nature, in advance of a government statement, were unhelpful. The Ministry suggested a confidential discussion with LCC officers on post-war hospital policy, and the possibility of forming a London regional council. Latham was briefed by the Clerk and Allen Daley, who had succeeded Sir Frederick Menzies as medical officer of health. Daley had taken over in 1939 and was a different type of man. He was a superb administrator with demoniac energy, but he had a smoothness of manner which made him easy to work with. One administrator who knew him said that, had he not been medical officer of health, he might easily have been the clerk to the council. The county council’s officers thought that a regional council involving over sixty local authorities was a daunting prospect, and the Clerk thought that much time would be wasted in debate. As a regional council would need supporting staff, would it not be better to have the staff without the council? Officers could outline principles and draw up a plan to guide decisions when the voluntary or municipal hospitals were seeking money. The council’s officers thought that an officer group would inevitably have to work closely with the LCC, and would absorb LCC thinking. Lord Latham would have preferred a simple LCC takeover of those voluntary hospitals which were needed, but his officers pointed to the strength of the opposition to be faced. The council therefore decided to develop a London County Council view of a ‘regional scheme’, and also to continue to plan a comprehensive service for the administrative county including cooperation with the larger voluntary hospitals. The Ministry was told that the London County Council thought that a regional council would be a waste of time. Instead the Ministry might second an officer to conduct a hospital survey. This course of action would be acceptable to all and would bind no one. Planning could be based upon such a survey, and the London County Council might be willing to aid voluntary hospitals which were part of such a plan, if the council had representation on their management committees. On 9 October 1941 the Government made an announcement in the House of its postwar hospital policy, and the decision to institute a hospital survey for London to provide a firm basis for planning.13The Minister’s statement proposed a service organised by local authorities, in which the voluntary and municipal hospitals would cooperate. There had been careful drafting and an attempt had been made to avoid antagonizing any group more than was inevitable. A sentence was inserted at the last moment which said that special arrangements were contemplated for teaching hospitals, in the way of increased educational grants. The word ‘regionalisation’ was studiously avoided, but the Minister indicated that the service would have to be designed with reference to areas considerably larger than those of individual local authorities. There was advance consultation with the local authority associations, which welcomed the announcement. Afterwards the Ministry of Health held separate meetings with the local authorities, the medical profession and the voluntary hospital movement. The latter disliked the idea of a service under local authority control and the proposed financial arrangements; they began to mobilise their opposition. In January 1942 Dr Allen Daley met the surveyors the Minister had appointed for an exchange of views.14 He explained the position of both parties on the London County Council. They favoured a county hospital service standing on its own feet, and not in any position of inferiority to the voluntary hospitals. The majority party was opposed to any organisation of hospital services on the basis of charity, believing that hospital services should be given to every ratepayer as a right. They were however softening their line on grants to the voluntaries, and might be disposed to accept a plan on something like the following lines: 1. The survey of the hospitals which was to be carried out would show the number of patients from the area of the London County Council which were treated at the voluntary hospitals, and the proportion of their beds which might be regarded as ‘London beds’. These beds could be included in the county council’s service, as long as they were in hospitals which the survey had recognised as efficient units. 2. The London County Council would make a contribution towards the cost of these beds, perhaps on a patient/week basis, at a level set below the average cost in the council’s own acute hospitals. Voluntary hospitals participating in such a scheme would have to agree on the rates of pay of their staff, a roughly uniform basis for the levying of patient charges, and to accept London County Council representatives on their committee of management. 3. The council’s payments would have to be made to the individual hospital, and not to a central body like the King’s Fund or the Voluntary Hospitals Committee. The London County Council was in favour of the disappearance of many of the special hospitals as independent units, on the ground that they were too small to provide proper facilities or employ satisfactory staff. Perhaps they might amalgamate with large neighbouring general hospitals, whilst the big special hospitals could remain independent, although linked for postgraduate teaching to the postgraduate school. The LCC also wished to play a larger part in undergraduate teaching, linking hospitals to provide clinical material. A degree of centralisation of services was also called for; certain forms of treatment like neurosurgery or deep X-ray therapy should not be provided at every existing teaching hospital.12,14 Planning initiatives The Minister’s statement to the House in October 1941 [13] stimulated a number of groups to begin work to ensure that their interests were not overlooked. The Leader of the London County Council instructed his officers to produce proposals for the administrative county. The voluntary movement began to take stock of its position; and the Ministry survey of the home counties was set in motion. Shortly afterwards at the government’s request Sir William Goodenough began to examine the problems of medical education in a national context. Even before the Minister’s statement, the British Medical Association, the three Royal Colleges and the Society of Medical Officers of Health had been considering the establishment of planning committees. The British Medical Association was early off the mark and invited the others to join in. Acceptable arrangements being agreed, a single commission was formed in May 1941, of which Lord Dawson was a member. Sir Harold Himsworth, later secretary of the Medical Research Council, said that the meetings were a stimulating mixture of realism and idealism, seen at its clearest in the interim report, produced in 1942 after a series of plenary meetings.15 It was a remarkable and radical document, in which the more controversial proposals were only agreed after hard-fought discussions. It is doubtful whether the report as a whole carried the support of all sections of the committee, indeed the medical officers of health produced their own document. But the profession appeared to accept not only the notion of a comprehensive health service in principle, but to foresee the nature of the changes which would have to come about. Amongst other recommendations the report accepted the need for new local health authorities, serving a population of at least half a million, advised by medical advisory committees to which professional problems would be referred. The joint coordinating committee The King’s Fund and the Voluntary Hospitals Committee established a joint coordinating committee soon after the Minister’s announcement to the House. It first met in November 1941 to consider regionalisation and the repercussions this might have on London’s voluntary hospitals, for the Nuffield Trust’s moves were not without their dangers. The establishment of self-contained regions in the home counties might lead to a clash with London on issues such as cases for teaching hospitals, appeals, and contributory schemes. Neither was it clear that London would fit neatly into the Nuffield pattern of regions and divisions. At fortnightly meetings the committee discussed how ‘adequate provision of the best possible treatment’ could be achieved.’6 It rapidly concluded that the area to be considered was the counties of London, Essex, Hertfordshire, Middlesex, Kent, Surrey, and probably East and West Sussex and south Buckinghamshire. However the voluntary hospitals in the home counties had misgivings that their interests might be adversely affected by the work of a London-based committee. In January 1943 representatives of the home counties were therefore invited to join the committee. Once the Ministry’s survey was under way attention was turned to the definition of an ideal form of teaching hospital. The conclusion was that it should have at least 750 and preferably 1,000 beds, possibly achieved by grouping hospitals together. Medical staffing, and special hospitals, were examined at some length. The Sankey Commission had been critical of the special hospitals but a united front was now required, and the committee asked each one the part it would wish to play in a coordinated service in London. The private view of the committee members was that whilst there was scope in London for those which had established an international reputation by their work, with the exception of the maternity hospitals there was no room for more than two in each specialty, and that these should be of university standard with at least 100 beds. Smaller hospitals might be associated with a neighbouring teaching hospital. However these robust sentiments were softened a little when, in July 1943, the joint committee’s interim report was drafted.17 The survey the Minister had announced was undertaken by Dr Archibald Gray, an eminent dermatologist, a senior member of the London Voluntary Hospitals Committee, Dean of UCH and President of the Royal Society of Medicine. He was assisted by Dr Graham Topping, deputy medical officer of health of the LCC. Gray had an unassuming manner but an impressive grasp of medical administration and wide contacts through the King’s Fund and the University of London. He could select the key issues for which a solution was required and much of the thinking behind the survey was his. Topping was something of a cynic, who had been heard to say that the council’s hospital service was the best of its size in the world. John Pater, from the Ministry, acted as the secretary, and the team worked well together, visiting virtually every hospital in the south east of England. The survey was designed to collate the facts about existing and prewar hospital accommodation, including a description of the available hospitals, the clinical conditions treated, the geographical origin of patients, and the relationship of supply and demand for hospital facilities. The surveyors were asked to advise on the role of each hospital, those which were redundant, the places where new accommodation was required, and the ‘area surrounding London which would appropriately be served by a hospital system centred on London, which would fit in with other areas so as to form part of a comprehensive scheme covering the whole Country’.14 They were not to consider political matters, like finance or the pattern of the administrative structure, but medical issues—the services which could be provided within a locality and those which should be based upon a distant centre. The King’s Fund had been planning to send a questionnaire of its own to the voluntary hospitals to determine their views on regionalisation. It now offered the draft to the surveyors, and after amendment this was sent out to all hospitals in the London area, both municipal and voluntary. Copies also went to hospitals outside the capital, although the covering letter they received suggested that the primary concern of he surveyors would, no doubt, be hospitals within the Metropolitan Police District - the area of the King’s Fund. Both the King’s Fund and the London County Council were involved in the mechanics of the establishment of the survey. They were provided with the draft terms of reference and the surveyors’ instructions. The council suggested amendments, as it wished to get away ‘from the crisp (and to our way of thinking) dangerous phrase “London Hospital area”.’ The instructions to the surveyors remained confidential; neither was it proposed to publish the final report, partly to enable the Ministry to keep a completely free hand on questions of major policy, which might include matters like the removal of hospitals from London.14 During the first part of 1942 the area covered by the London survey was enlarged; some counties were asking for their services to be surveyed alongside those of London, and the British Hospitals Association and the Nuffield Provincial Hospitals Trust acted as the surveyors’ agents in obtaining data on hospital facilities and catchment areas in the home counties. In October the extension of survey was announced formally. The press began to take an interest. ‘LONDON’S LITTLE HOSPITALS DOOMED’ ‘The majority of the capital’s smaller establishments will disappear after the war. That is the view of the medical experts representing both municipal and voluntary hospitals, appointed by the Ministry of Health ... “We have found that both municipal and voluntary hospitals are today collaborating and doing a first class job of work”, one of the experts told the Evening Standard. But the smaller unit is not nearly so suited to modern hospital treatment as the big establishment, both economically and administratively.’ Evening Standard, 7 May 1942 ‘HOSPITAL SYSTEM THREATENED’ “‘So far as I can make out”, said Viscount Davidson, “a vast amount of planning is going on. But it is being done by those who have no urgent desire to see the voluntary system preserved, or by those who are eager to see it destroyed”.’ Daily Telegraph, 28 October 1942 By the end of 1942, other hospital surveys were being established under the auspices of the Nuffield Provincial Hospitals Trust, and meetings were arranged between the surveyors to discuss the survey boundaries. The extension of the London survey outside the Greater London area led the voluntary hospitals in the home counties to fear that the fate of the hospital services in their areas would be decided by ‘a London committee’. The King’s Fund and the Voluntary Hospitals Committee therefore widened the membership of their joint coordination committee to include representatives from the home counties. The Ministry was also asked what the consultative procedures would be when the survey was complete. The Fund was told that the factual information and the Minister’s decisions would be published, but the surveyors’ advice to Ministers would remain confidential. As the months passed the London survey area continued to expand, and Dorset and Bedfordshire were taken on at the end of 1942. The White Paper on a National Health Service (1944) The preliminary results of the hospital surveys were already available to those drafting the White Paper on a future national health service and it was apparent that in many areas the hospital services were badly coordinated. Organisation was therefore to be based on ‘joint authorities’, joint because county and county borough councils would be grouped together for efficient management. [See a pamphlet on Health for All]
Municipal hospitals serving a county town, and those serving the surrounding countryside, were often managed independently and restricted to one or other group of ratepayers. However the White Paper accepted that in London no combination was necessary, and the existing authority would be able to undertake the new functions.18 Plans would in future be prepared for a comprehensive service, and be subject to ministerial approval. The voluntary hospitals would remain as independent contractors, free to participate in the scheme if they wished. The London County Council welcomed the White Paper, and the recognition that the county council should act as a single unit within the comprehensive medical service proposed. The British Hospitals Association and the King’s Fund were, to put it mildly, unhappy.19 They saw no sign of a partnership if the responsible authority was to consist entirely of the elected representatives of local government. The British Hospitals Association thought that the White Paper proposals left the voluntary hospitals a wholly inadequate voice in planning and administration. Instead of joint boards, the Association argued for regional councils, each region to include at least one teaching hospital. Finance being the touchstone of independence, the voluntary movement wished to see a continuing income from voluntary sources, and the scheme did not seem to make this practicable. The London County Council, for its part, objected to any suggestion that the managing committee of a National Health Service area should have any non-elected members representing specific interest groups, like the doctors. Increasingly there was pressure for the publication of the survey. In April 1944 Kent County Council asked for details of the survey, so that its own hospital planning would not proceed on lines incompatible with a wider scheme of things. In reply Mr Pater made ‘ few rambling remarks’ which indicated the lines upon which the surveyors had proceeded in delineating districts: ‘In the first place they mainly follow existing local Government boundaries; this was done merely to make it easier to arrive at an estimate of the population to be served and not because the boundaries are regarded as lines which patients should not, and will not, cross. Secondly, the districts were defined having regard to transport, density of population and so on, in order to provide a population and an area which could be reasonably expected to support a large and efficient district hospital. By this is meant a hospital with the normal range of special departments staffed by specialists and consultants and catering for maternity, fevers and the chronic sick in the sense of the bed-ridden as well as for general and special acute work. It is assumed that even these district hospitals may not stand on their own legs for all normal purposes but may, for exam look to a neighbour to supply beds for skin or eye cases. It was agreed that the survey should be made public. Hospitals wrote in for advice on postwar planning; the Soho Hospital and the Samaritan Hospital were considering amalgamation—how would this fit in with plans? The Ministry and the surveyors found themselves having to respond helpfully and the only document available to them was the draft of the hospital survey. Dr Gray submitted the survey to Sir John Maude at the Ministry on 29 April 1944. He pointed out that the factual material had been collected before the most recent series of air-raids on London and south eastern England, which had led to further damage to hospitals, and that the second part of the document had been drafted in advance of the proposals of the 1944 White Paper, and without knowledge of what they might be. However Gray did not believe that modifications were necessary or that there was any conflict of principle.20 It was generally known that the survey was complete. A continuous stream of letters was received by the Ministry from local authorities and hospital managers who wished to plan hospital developments, and who wanted to know how the surveyors had regarded the local services. Under wartime conditions it was difficult to get the survey printed, and the Ministry advised correspondents to delay action until it was available. The publication date was postponed first until Christmas 1944 and then to the New Year. In any case it became clear that the survey could not be regarded as the last word on hospital planning. The Minister wrote to one correspondent in January 1945 that ‘the suggestions made in it are not, of course, final, and future action will depend amongst other things on the Government’s general proposals for the health service’. People were therefore advised not to launch into schemes which might not be in the best interests of good hospital services until they had read the survey.20 The survey was finally published in April 1945 while the debate on the proposals in the White Paper was still in progress.21 It created little stir, for most people were far too bogged down in national issues to worry very much about its contents. A series of categories had been devised and hospitals, or those proposed for the-future, were allocated to one or other of them. Similar classifications later appeared in the surveys of other parts of the country, and most groups of surveyors recognised the following: a. Regional university centres providing both local district services and regional units for plastic surgery, thoracic surgery, radiotherapy and neurosurgery. Most regions had only one of these centres, but some like London and the north western region had more. b. Local cottage hospitals staffed by general practitioners with varying levels of visiting consultant support. These were uncommon in central London but were found on the outskirts. c. An intermediate category of divisional, area or district hospitals providing all day-to-day services with full time resident staff and cover from consultants living nearby. While the surveys had been in progress an attempt was made to develop a common terminology and Sir Wilson Jameson took a personal interest in their progress. The London surveyors provided an indication of the type of district hospital they thought appropriate to a densely populated area. They estimated that an urban district with a population of 120,000 might support a hospital of 650 beds containing:
There would also be 150 beds for the chronic sick, but dermatology, genito-urinary and ophthalmic work would be sited at selected hospitals only; otherwise the size of the units would be too small. In general, the hospitals would be about 800 beds in size, neither larger than 1,000 nor smaller than 400, serving a district of 100-200,000, a range of size which was larger than most of the voluntary hospitals. The surveyors thought that the smaller local hospitals had little part to play in densely populated areas. Special centres serving wider areas would be required when a high degree of concentration of equipment or staff was necessary for maximum efficiency.21 Authority boundaries The parallel provincial surveys had been organised by the Nuffield Provincial Hospitals Trust and a number of them proposed that services should be organised on a regional basis. These surveys often defined the boundaries of the region and indicated its centre, the town in which the university teaching hospital was situated. In London the surveyors were silent on such issues. The Minister had asked them to state the area which would be appropriately served by a hospital system centred on London but they did not do so and nobody was very surprised. While the boundaries of most regions in the provinces were pretty obvious that was not the case in the south-east and Topping might have been out of a job had the surveyors disregarded the London County Council’s opposition to regionalisation. Geographical areas were a political matter to be fought out at a higher level. District boundaries were less contentious, although in London the areas served by the hospitals generally overlapped and the movement of patients was often determined by features like the Thames, the Hackney marshes and the radial network of railways. In general, the surveyors said: ‘Each county area has been divided for planning purposes into a number of districts suitable according to size, population and transport facilities to be served by a district hospital. For practical purposes the boundaries of these districts normally follow local authority boundaries; but we fully realise that in practice the boundaries between hospital service areas will be indistinct and may not coincide with administrative boundaries. We assume that present or future boundaries will not be permitted to interfere with the flow of patients according to their needs.’ The effect of bombing on the hospital services of the capital was found to be considerable. The surveyors estimated in 1943 that 3,000 beds had been lost in general hospitals within the London County Council area, and more were subsequently lost in the flying bomb and rocket attacks of 1944. Major damage had been sustained by both the voluntary and the municipal hospitals, and while hospitals like The London and St Thomas’s were instructing architects to prepare plans for reconstruction before the war in Europe had ended, the gains by wartime rebuilding were small. A major virtue of the survey of the London area was that it presented an overview of hospital facilities throughout the south-east of England which was detailed, consistent from area to area, and supported by factual information derived from analysis of the questionnaires. Conceptually, the surveyors selected from the ideas already under discussion, pulling them together into clear and concrete proposals. The survey remained an essential tool for hospital planners until the publication of the Hospital Plan in 1962. The surveyors adopted a norm of five acute beds per thousand population and assessed local deficiencies against this. As had been the case for many years, provision was worst in south London, especially in Lewisham and Wandsworth. Ealing, Finchley, Harrow, Tottenham and East Ham also had problems. As a whole however, as Burdett had said in 1903, the area of the London County Council was adequately served; it was the distribution which was poor, with comparatively few facilities at the periphery. To make this good the surveyors envisaged a first phase of short-term measures, often involving a degree of overcrowding, followed by longer term schemes as labour and building materials became available. Recognising the movement of the population from the centre of London, and the likelihood that this would continue, they recommended that the question of hospital building in London be ‘approached with circumspection’, apart from making good war-damage by temporary repairs.2’ Most of the proposals for major development were for the home counties. In Middlesex they suggested a new hospital at Harrow, rebuilding at Hillingdon, extensions at Ealing and a new hospital in Enfield. In the London County Council area they believed that new hospitals should be provided in Tooting and Sydenham. New hospitals being required on the outskirts of London, they suggested that three teaching hospitals should move out. It was proposed that Charing Cross Hospital should move to Harrow, St George’s to Tooting, and the Royal Free to Highbury. During their visit to the Royal Free Hospital the surveyors had touched on the idea of removal, and when a bomb subsequently fell on the hospital, matron blamed the surveyors. Sir Archibald Gray, coming from University College Hospital which had itself taken over a number of small hospitals, saw no reason why the same should not happen to others. The survey suggested that the special hospitals should either be closed, amalgamated with undergraduate teaching hospitals, or rebuilt on a site near the University. As the years passed, Gray said, those who had opposed amalgamation gradually retired. Death, he said, was a great healer; and as he was also a member of the Goodenough committee on medical education it is not surprising. The reaction to the survey The survey was not to everybody’s liking and some were incensed to find that their local hospital was marked down for closure. Others wrote to correct minor factual errors. St Monica’s Home Hospital, Brondesbury Park, the Hospital of St John and St Elizabeth and the Weir Hospital protested that their facilities had been criticised unreasonably. Croydon General requested a ‘re-survey’ as they disagreed with the surveyors’ comments that they were on a restricted site. They already had plans to double the number of beds. Battersea General and Wandsworth Borough Council also protested.20 The Ministry replied that the survey was the personal view of those conducting it. For the present the Minister did not propose to indicate his views on any individual proposal, but that did not stop some from acting upon its recommendations. Westminster Hospital began negotiations with the governors of the Infants Hospital and it was agreed that the institutions should merge. The surveyors had laid out the pattern of a coordinated hospital service for London and the home counties, district by district. Some might not like the pattern, but it lay to hand for the use of those whose job it would be to take matters further. The voluntary hospitals’ planning The joint coordinating committee established by the King’s Fund and the Voluntary Hospitals Committee issued its own report on postwar hospital problems in London and the home counties after the London hospital survey and the Goodenough report on medical education had appeared.22 The members of the committee had kept in close touch with the Nuffield Trust and the chief medical officer, Sir Wilson Jameson- who they thought were in sympathy with their views. The joint committee’s report outlined a future hospital service as the voluntary movement would like to see it, largely rejecting the surveyors’ criticisms of inequitable distribution of hospital staff and facilities. The committee opposed the idea of a single system, believing that standards were maintained by competition, and the voluntary hospitals provided the standard by which public hospitals could be judged. It viewed freedom of choice by patients as essential, wished the London region to be extended to include the home counties, and to see the influence of the University of London reach out until ‘the area of influence of other universities was reached’. Some faults of the voluntary system were admitted and remedies were suggested. Too many voluntary hospitals were small, ifi-equipped and could not accept the whole range of acute work in their locality. Medical and nurse staffing needed overhauling, but while a hospital of under 150 beds could not provide full general hospital services, there ‘lurked a danger that arguments in favour of a large hospital could be carried too far’. Smaller hospitals possessed advantages, they served a more local population, were well known to patients: and could ensure a friendly personal atmosphere. ‘Very large hospitals could easily become the coldly efficient kind of institution, so terrifying to the sensitive.’ The joint coordinating committee believed that there was little justification for hospitals of 100 beds or less; these should amalgamate or move to the periphery. In the ‘industrial and dormitory zone’ an ambitious programme of voluntary hospital development should be encouraged, and in the home counties the municipal hospitals and the voluntary hospitals should build up links through joint staff appointments. The Inter-Departmental Committee on Medical Schools23 The presence of a medical school had always had a significant effect on the hospital to which it was attached, but educational factors as such had had little effect on the hospital system until the inter-war years. Thereafter there was increasing appreciation of the special nature of teaching hospitals, and academics were more frequently in evidence on major policy-forming committees. The Goodenough committee was established in 1942 in the wake of the announcement of the government’s post-war hospital policy.24 This had suggested that special financial arrangements might be needed to assist the teaching hospitals, and it was decided to set up an advisory body to consider this, amongst many other issues. The committee was a classic example of how to get the recommendations wanted by handpicking the members who were going to make them. Wilson Jameson took a leading role in the selection of a committee which was likely to suggest a much wider admission of women to medical schools, a larger development of professorial units particularly in London, and the abolition of non-university medical education. There were two representatives of UCH, which had the most highly developed professorial system of all the medical schools of London, including the dean, Dr Archibald Gray. Wilson Jameson was himself a member, and the chairman, William Goodenough, had an excellent grasp of hospital problems as a result of his work at the Radcliffe Infirmary and the Nuffield Provincial Hospitals Trust. The secretary to the committee, Farrer-Brown, was already well known to him. The committee first met on 14 April 1942 to enquire into the organisation of medical schools, particularly in regard to facilities for clinical teaching and research’. While much of the committee’s remit was national in nature, its attention was directed at the outset to two London problems: the organisation of pre-clinical teaching, and the possible amalgamation of the smaller clinical schools. It was suggested that schemes for coordinating hospitals would make the continued existence of the small schools as completely self-contained and independent units unnecessary. Coordination of hospitals would also make it possible to link hospitals for teaching purposes so that a school, while primarily associated with one hospital, would be able to call upon the facilities of others. The Goodenough committee took a wide range of evidence, consulted all medical schools and professional organisations, was invited to visit the London County Council hospitals, and explored their educational potential. Few things in London are secret, and the county council’s officers received covert copies of the committee’s papers.25 Dr Somerville Hastings, Mr Reginald Stamp and Lord Latham all wished the council to play a larger part in medical education, perhaps by the establishment of a municipal teaching hospital if recognition by the General Medical Council could be assured. The council gave evidence on undergraduate medical education in November 1942 and on postgraduate education in February 1944. Pointing out that it was the largest single civilian employer of doctors in the country, the council wanted medical education to cover a wider range of subjects in the future, including preventive medicine. The council suggested that its hospital service could provide an excellent and complete medical training, were it to become the basis of a medical school. Such a school might be established at one of its larger hospitals, using the others as required.26 The council pointed out that it already supported the Postgraduate Medical School at Hammersmith. Behind this proposal lay a hope that the London School of Medicine for Women might leave the Royal Free Hospital and attach itself to the Highgate group of hospitals. Witnesses were questioned about the number of beds required to teach an intake of 100 clinical students. The British Medical Association’s memorandum of evidence was the most specific on the subject, and Professor Henry Cohen, from Liverpool, explained how the Association’s figures had been worked out. The Goodenough committee found that there was a wide measure of agreement with Cohen’s estimate, and the table presented in the report is substantially the same as the guidance of the University Grants Committee in 1976, thirty years later. The British Medical Association saw no reason why a local authority hospital of the requisite standard should not be the ‘parent hospital’ of a medical school.
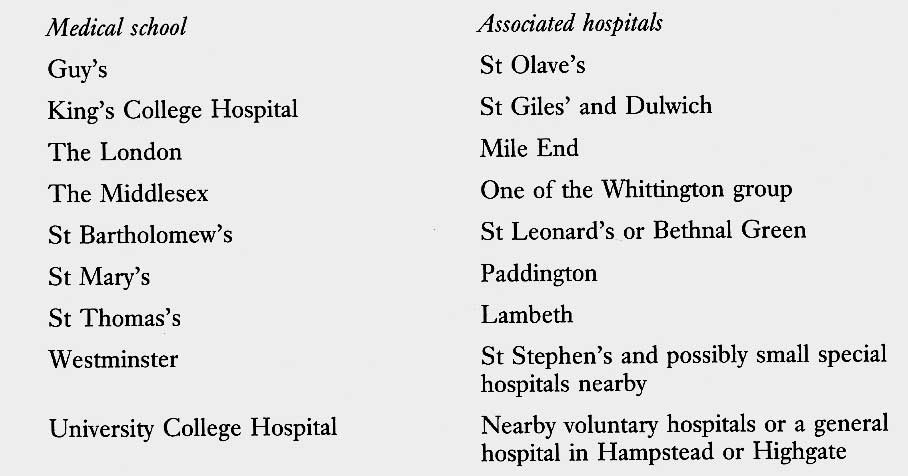
The Goodenough report was published in 1944 and was the most important statement on medical education since Sir George Newman’s Notes on Medical Education (1918). It provided a clear statement of the aims and methods, and how these might relate to a national health service. The report recommended that medical education should become more educational and less vocational in nature. Every medical school should be a university medical school, and an integral part of a university. In London, only two were independent bodies - St Bartholomew’s and the London Medical School for Women; all the others were ultimately under the controlling power of the governing body of the parent hospital. The committee believed that teaching hospitals should be full partners in the hospital service of the district in which they were situated, but saw that the population of central London would become less and less able to support the needs of medical education. Underlying the recommendations lay the concept of a university medical teaching centre, consisting of a university medical school and a group of teaching hospitals, one parent hospital to which others were associated. By the standard it set, based on Cohen’s figures, ten of the medical schools were short of medical beds, and seven of surgical beds as well. Goodenough saw the need to expand the medical intake. But the number of medical schools in London was large, possibly too large. The report recommended that the West London Hospital Medical School, which had assisted since 1937 with the education of women, should close.27 Instead it was suggested that exchequer grants to medical schools should be dependent on a policy of coeducation. It was proposed that specific municipal hospitals should be associated with nearby parent teaching hospitals, that Charing Cross Hospital and its school should be moved to a site in Middlesex, St George’s to another outer suburb, possibly in south London, and that the Royal Free Hospital should move to a northern suburb). Associated hospitals for medical schools
While educational purposes might best be served by concentrating schools in central London, the future hospital requirements of London seemed unlikely to justify the continued existence of all the teaching hospitals in the middle of town. An outward movement seemed inevitable, and was not without educational advantages. Charing Cross and St George’s had raised the possibility of relocation in their evidence to the committee and it would provide breathing space for the other teaching hospitals. The amalgamation of the smaller schools was considered, but the balance of opinion was against the proposal, favouring the transfer of entire institutions to the periphery. When implemented, this recommendation had the effect of re-establishing preclinical departments at two hospitals which had lost them prior to the First World War. Goodenough saw no reason in principle why a municipal hospital should not form the basis of a medical school; but in London medical schools were already too numerous to warrant an addition to their numbers. Expansion of existing schools seemed preferable and one possibility might be to use a local authority general hospital as the basis of an existing medical school which would be relocated. The members and officers of the London County Council considered these recommendations carefully, discussing them with Sir Wilson Jameson and representatives of the voluntary hospitals. The Council decided to cooperate, where possible on a basis of equality, in the provision of teaching facilities, rather than press its claim to its own teaching hospital. The alternative was to criticise the Goodenough report, to include a teaching hospital in its own plan, and to fight for it. Reginald Stamp, for the Council, thought that this was not the best tactic, because the Council would find itself planning London’s health service with the voluntary hospitals and the doctors ‘in the wrong mood.25 While ‘association’ carried the risk that all the interesting and acute cases would go into the parent teaching hospital and not the municipal one, the cost and complexity of developing a teaching hospital was considerable. Finally, the Goodenough report concluded that there was a need to organise and develop facilities for postgraduate education. The London County Council’s hospital planning Responsible as it was for three-quarters of the hospital beds in London, the council was making its own plans.28 Daley, who had now received a knighthood, was respected in voluntary hospital circles, as Sir Frederick Menzies had been. He was frequently invited to discuss hospital problems. At the request of the chairman of his committee, the structure and staffing of the LCC hospital service was reviewed. The medical superintendents of the council’s hospitals discussed reports like that of the Medical Planning Commission as they appeared and the superintendents were asked for their view of the internal administration of the hospitals, their staffing, size and medical advisory committees. Sir Allen Daley kept himself well informed about the progress of the London hospital survey and the work of the Goodenough committee. He was invited to St Mary’s to speak about the probable attitude of the county council to the voluntary hospitals, and to St George’s to consider its possible relocation in south London. His draft plan for the council hospitals was prepared towards the end of 1945, after the other reports had already appeared. Commenting upon Daley’s plan, Mr Reginald Stamp, chairman of the LCC Hospital and Medical Services Committee, suggested that Daley had paid too much attention to the hospital survey, on the assumption that it would command a greater measure of support than was likely to be the case. He had also shown a tendency to accept the voluntary hospital point of view, ‘rather than indicating what was or could be the best proposals to provide an improved municipal service’. Daley pointed out that the survey had in fact been published by the Ministry of Health, and even though it was the work of independent surveyors, it was inevitably going to be regarded as a key document. In November 1945, Sir Allen Daley sent the final version, which was to go to the committee, to Sir Arthur Rucker, Deputy Secretary at the Ministry. The London County Council plan was consistent with the recommendations both of the hospital survey and Goodenough, and proposed a series of main hospitals of 400—1,000 beds linked with smaller hospitals nearby. The administrative county was divided into twenty-one districts, in line with the neighbourhood units of the County of London plan. In eleven of them the main hospital would be a municipal one; but in ten in the centre of London it would be one or more of the teaching hospitals, linked to municipal hospitals by staff-links..29 LCC Hospitals identified as "main hospitals."
Daley thought that the pre-war total of beds was adequate but that local shortages would have to be remedied by new building, including a new main hospital at Tooting, one in the Crystal Palace area, considerable development of the Fulham Hospital, and ‘certain integrations of the Archway group’. The outpatient departments in many of the LCC hospitals were regarded as inadequate as the old infirmaries had never developed this service to the same extent as the voluntary hospitals, although some voluntary hospital staff like Lord Dawson undertook regular clinics in municipal hospitals. This shortcoming would be remedied, and appointments systems would be introduced as soon as possible. It was suggested that ground should be bought near hospitals with restricted sites; some hospitals were listed for closure. Sir Allen Daley drew attention to the considerable expenditure by the Council since 1934, but a major capital programme was clearly required. The Comptroller of the Council believed that the new proposals were difficult to cost, and it would be some time before the more ambitious features of the programme could be carried out. The report covered specialties like radiotherapy, plastic and thoracic surgery, problems of medical and nurse staffing, and administrative matters. It reiterated the London County Council policy of centralisation. ‘The Council, since its creation, has for very good reasons attached great importance to the principle of central control in all major matters. This principle ... has necessarily imposed limits on the autonomy of various local institutions and services.' Nevertheless both Sir Allen and the council were anxious to do everything possible to foster the individuality of hospitals subject to the overriding goal of a hospital service for London and the Londoner. Sir Allen thought it inappropriate to re-examine the policy of centralisation until the government had announced its policy on a national health service. However, he proposed improved medical advisory machinery and believed that thought should be given to allowing hospital committees a small budget to dispose of as they wished, up to a maximum of £200 per year in the larger hospitals. The report concluded with 43 recommendations. It is of particular interest for the tables and appendices which provide a bird’s eye picture of the London County Council hospital service, and an insight into how the National Health Service might have developed in central London had its management fallen to the county council. On 27 November 1945 the LCC Hospital and Medical Services Committee referred it to the council’s finance committee. It was considered again in December and the views of the medical officer of health were generally endorsed. The report was then referred to the council with an indication that the government proposals for the health service were awaited. In the meanwhile, it was suggested, the various proposals might be the subject of specific reports with estimates of cost. The council received a shortened version on 19 February 1946 but gave no instruction for specific action to be taken.30 The report received a mixed press. The Lancet said that it made stimulating reading, and welcomed the possibility of expenditure on the hospitals. The Medical Officer said that it was clearly a long term plan. The Economist thought it might soon be outdated, and that continuing to pay the medical superintendents of council hospitals more than clinicians would deter many clinicians from joining the council's service. The Economist was right; the publication of Aneurin Bevan’s proposals outdated the plan very soon indeed 1 The emergency hospital scheme. Lancet, 1939, ii, p 938. 2 PRO/MH/76/128. 3 King’s Fund A/KE/222. 4 Cameron H C. Mr Guy’s Hospital. London, Longmans Green and Ca, 1954; Clark-Kennedy A. The London. London, Pitman, 1963; and organisation of a sector. Lancet, 1939, ii, p 758—9. 5 Dunn G L. The emergency medical service, vol 1. London, HMSO, 1952; and Hospitals in emergency. Lancet, 1939, i, p 723. 6 The emergency hospital scheme: political and economic planning, 1941. vol 8, no 177. Lancet, 1941, ii, p 413. 7 London County Council papers. PH/HOSP/4/42. 8 Pater J. The making of the National Health Service. London, King Edward’s Hospital Fund for London, 1981. 9 A general medical service for the nation. London, British Medical Association, 1930 and 1938. 10 Taylor S. A plan for British hospitals. Lancet, 1939, ii, p 945; and A plan for Britain. Picture Post, January 1941. 11 PRO/MH/80/24. 12 PRO/MH/77/25. 13 Parliamentary Debates (Hansard), House of Commons, 9 October 1941, columns 1116—18; and Hospitals first. Lancet, 1941, ii, pp 455, 466. 14 PRO/MI-I/77/1 and PRO/MHI8O/24 (preliminary papers on NHS Bill). 15 Medical Planning Commission. Draft interim report. London, BMA, 1942; and Lancet, 1941, ii, p 347. 16 King’s Fund A/KE/95; and A/KE 96. 17 King’s Fund A/KE/17; and A/KE/101. 18 Great Britain, Ministry of Health and Department of Health for Scotland. A National Health Service. London, HMSO, 1944. Cmnd 6502; and A/KE/355. 19 PRO/MH/80/34; and A National Health Service. London, British Hospitals Association, 1944. 20 PRO/MH/77/3. 21 Gray Sir A M H and Topping A. The hospital services of London and the surrounding area. London, HMSO, 1945. Ministry of Health hospital surveys volume 1. 22 Report of the Joint Committee on Postwar Hospital Problems in London and the Home Counties. London, King Edward’s Hospital Fund for London and the Voluntary Hospitals Committee for London, 1945. 23 Great Britain, Ministry of Health and Department of Health for Scotland. Report of the inter-departmental committee on medical schools. (Chairman: Sir William Goodenough). London, HMSO, 1944. 24 Parliamentary Debates (Hansard), House of Commons, 9 October 1941, columns 1116—18. 25 London County Council papers. Working papers of the Goodenough committee, File Series PI-L/HOSP/4/41 — 4/52. (For papers on a municipal teaching hospital see P/HOSP/4/48.) 26 Minutes of London County Council, 1942, pp 823—843. 27 PRO/MH/58/346; and Lancet, 1937, ii, pp 1038—9. 28 London County Council papers on the municipal hospital programme for London. PH/HOSP/1/4, 5, 6, 7 and 8. 29 Hospital and ancillary services — considerations affecting future developments, H & MS 813. London, London County Council, 1945. 30 The hospital service — future development. Report of the Hospital and Medical Services Committee. London County Council, February 1946; and PH/HOSP/1/8.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||