| The Smallpox Hospital | The risks from the hospitals |
| The London Fever Hospital | |
| The Metropolitan Asylums Board | References |
|
Fevers, including smallpox, typhus and enteric fever, were one of the greatest problems with which cities had to deal. The problems were made even worse by the arrival of cholera in London in 1832. The size of epidemics and the risk to the population led many cities to establish some form of ‘house of recovery’ or ‘pest-house’, but the size of London meant that the few facilities which existed were inevitably overstretched. At times of crisis the hospitals might admit some patients, others would be cared for in the workhouses, but many died or recovered at home. Those who were wealthy were invariably looked after at home, where they would be more comfortable and could receive better care, as well as being isolated from others. There was little agreement Within the medical profession about the best way either to treat patients or to organise care. In 1850 the General Board of Health commissioned a study into methods of prevention and treatment and whether the risks to the staff were least if patients were spread evenly throughout a hospital or were concentrated in a single block.1 The rules of many of the general hospitals excluded patients with fevers altogether, but hospitals varied in their admission policies, and would change their practice over the years. In 1746, by ‘the benevolence of a few generous individuals’, a charity was established to receive persons of all ages and denominations who were suffering from smallpox. The charity intended not merely to provide every facility for treatment, but also to study alternative methods of treating the disease. A house was taken in Windmill Street, Tottenham Court Road, and was soon filled. Others were procured in Coldbath Fields and Old Street.2 Expansion proved necessary and Rocque’s map of London (1769) shows the new smallpox hospital at Battle Bridge, where King’s Cross Station now stands. It was rebuilt yet again in 1846 as the London Smallpox and Vaccination Hospital on Highgate Hill in Upper Holloway and the building now forms part of the Whittington Hospital. Patients were admitted by presentation of a governor’s letter, or from the hospitals and workhouses of London on the payment of a fixed sum. Another voluntary hospital for infectious diseases (other than smallpox) was founded in 1802. It was originally established in Constitution Row, Gray’s Inn Lane, ‘to the great horror of the neighbours who threatened indictment and prepared for litigation’, and for a time it provided the main facility for fever patients for the whole of London. In 1815 the hospital shared accommodation with the Smallpox Hospital, moving into the west wing at Battle Bridge, where it remained until 1848 when the Great Northern Railway required the land. With the compensation received the hospital was rebuilt in Liverpool Road, Islington. Once more there was a public protest and Thomas Wakley was invited, as the local Member of Parliament, to address a meeting. Wakley used The Lancet to attack Dr Southwood Smith, physician to the London Fever Hospital, for supporting the governors in their plan to locate ‘a deadly pest-house’ for patients with the most malignant form of fever in the midst of a population of 60,000. The fact that Dr Smith was also the medical member of the new General Board of Health made his conduct, in the view of The Lancet, all the more reprehensible.3 In spite of the protests, the London Fever Hospital opened and it proved less of a hazard than had been feared. Most patients were admitted by parish order, at a cost to the guardians of one shilling a day. In its later history - after the Metropolitan Asylums Board was formed - the hospital concentrated on patients above the pauper class, servants of the upper classes and better-off people living alone. The charity found it hard to attract voluntary support and its patients - even if they survived - were not always good payers. Financial crisis was therefore commonplace. The Fever Hospital amalgamated with the Royal Free Hospital in 1948. The Metropolitan Asylums Board To the poor law fever hospitals belongs the distinction of being the first centrally planned hospital service in London. At times of crisis the London Smallpox Hospital and the Fever Hospital could not meet the demand. Parishes cared for patients in their workhouses, other buildings would be taken over, or tented hospitals would be erected. The unsatisfactory nature of this supplementary provision which depended on the varying policies of the different boards of guardians, was one of the problems solved by Mr Gathorne Hardy’s Act (1867). It created the Metropolitan Asylums Board, which consisted of 45 members representing parishes or unions and 15 from the central Poor Law Board. The new board assumed responsibilities from 30 boards of guardians which ‘could not be carried out by many independent authorities with varying needs and resources’. It was financed from a common metropolitan fund to spread the cost over rich and poor areas, based its policies on the professional advice it received, waged a running battle with the Poor Law Board, and came to be greatly respected. The new board began systematic planning as soon as it was established. To do so it needed to know the extent of the problem, so statistics of the deaths from fever in each parochial district in London were obtained for the previous years. The Poor Law returns from the workhouses, and the number of admissions to the London Fever Hospital, were also studied. The logic of the system was later explained to a select committee of the House of Commons by Dr Francis Sibson, consulting physician to St Mary’s and one of the central government nominees to the Metropolitan Asylums Board.4 The population of London at the time amounted to about three million and it fell into three main zones:
North Eastern District 967,000 The maximum distance it was thought wise to transport patients in an exhausted state from smallpox was three miles. As the diameter of London was about six miles a triangular system was devised with hospitals at the apices, six miles apart. A circle of half a mile was drawn around each angle, and sites were sought within these near Elephant and Castle, Victoria Park and Regent’s Park. Advertisements led to the offer of sites, but the Board had to proceed quietly and circumspectly for as soon as its interest was known there were protests from local residents. Sites had to meet several criteria. They had to be as near as possible to the great mass of the population without being within it, so that they enjoyed clean air; and the ground had to be about eight acres in extent. Sites had been located by early 1868, but in each case there was a deputation in protest. The Metropolitan Asylums Board therefore sought the agreement of the Poor Law Board to proceed, and this was granted. In each case the plan was to build a pair of hospitals, one for smallpox and the other for fevers. The architects’ plans can still be seen in the Public Record Office. The Homerton fever hospital was designed with one ward for scarlet fever, one for enteric fever and three for typhus. Building began at Homerton and Stockwell but construction at Hampstead was delayed at the suggestion of the Poor Law Board because the demand for accommodation was uncertain and it seemed reasonable to learn from the experience of the other two pairs of smallpox and fever hospitals.
However, events overtook the Metropolitan Asylums Board. An epidemic of relapsing fever in 1869 forced it to negotiate with the London Fever Hospital to erect a temporary ward at Liverpool Road, and to use the ground it had purchased at Hampstead. Two hundred and twenty men were put to work and within five weeks the green slope south of Hampstead Heath Station was covered by a hundred-bed hospital. It consisted of galvanised iron huts on a concrete base and included kitchens, accommodation for doctors and nurses, and a mortuary. It cost £8,000.5 The paired hospitals at Homerton and Stockwell were still not ready in 1870 when a very severe outbreak of smallpox swamped the existing facilities. The London Smallpox Hospital on Highgate Hill was quickly filled and many patients had to remain in the workhouses of the East End. More huts were erected at Hampstead to the increasing alarm of the residents. In February 1871 the construction work at Homerton and Stockwell was advanced enough for the accommodation designed both for fevers and for smallpox to be put to use to admit patients with smallpox. Ground for further hospitals was desperately needed. Part of the Lillie Bridge racing ground in Fulham was acquired for the Western Hospital, and at Hatcham, a market garden off the Old Kent Road for the South Eastern Hospital. In April 1871 the Admiralty granted temporary use of the old hospital ship Dreadnought. By May additional space was created by the erection of marquees in the grounds of the hospitals at Homerton and Stockwell. Another smallpox epidemic in 1877 again swamped the board’s accommodation. ‘It would seem’, said The Lancet ‘that the vastness of the metropolis and the incoherence of its government precludes it from taking advantage of the teachings of experience’. As a result of the shortage of hospital accommodation many deaths occurred at home. The Fulham and Deptford Hospitals, the latter in temporary wooden huts, opened in the middle of the crisis and by the end of the 1870s the Metropolitan Asylums Board had five paired hospitals, all on large sites. Yet accommodation proved inadequate once more in 1881. Tents were erected for convalescent patients at Darenth and the Admiralty lent the battleship ‘Atlas’ for conversion into a floating hospital. This was positioned at Greenwich and later moved further down river.
A proposal to build a fever or smallpox hospital invariably led to protests from local residents, but at first there was little evidence that the hospital harmed the health of a locality. From the outset the inhabitants of Hampstead, led by Sir Rowland Hill, fought against the admission of cases of smallpox. The result was an enquiry into the Hampstead Hospital by a select committee of the House of Commons in 1875.4,6 Evidence showed that patients had communicated with people over the walls and that ambulance men and relatives called at The George, which still stands on Hampstead Hill, for refreshment. The committee concluded that the Metropolitan Asylums Board had acted properly and that such risk as there had been was due more to individual carelessness and poor control of patients - caused by crowding in an emergency - than to the presence of a smallpox hospital in the community. The board did in fact take all reasonable precautions and the regulations of the hospitals were severe. When a new ambulance station was established at the Eastern Hospital, providing accommodation for nurses, coachmen and male attendants as well as the ambulances and horses, the British Medical Journal praised the regulations. ‘At the hospital the ambulance is unloaded and then thoroughly disinfected; the nurse changes her outer clothing, and all blankets are left at the hospital for washing. After this the ambulance returns to the station. Besides this disinfection at the hospital we are informed that the nurses and officers bathe and change their clothes before they are allowed any leave of absence. There is not much fear, we apprehend, of the station becoming a centre of infection.7 Nevertheless there was increasing anxiety that the incidence of smallpox was higher in the vicinity of the smallpox hospitals. In December 1880, the Local Government Board, learning that the Fuiham Hospital was about to be used for smallpox cases, asked Mr W H Power, a medically qualified inspector, to enquire into the matter.8 He showed that there had been a marked change in the local distribution of cases each time the hospital had admitted smallpox. The nearer a household was to the hospital the more likely it was to suffer from the disease. Evidence was accumulating that there were dangers in siting smallpox hospitals in residential neighbourhoods and in 1882 the House of Lords settled a lengthy legal action in favour of the Hampstead residents.9, 10 A thorough and independent investigation was called for and the Local Government Board applied for a Royal Commission to examine the whole subject of hospital accommodation for infectious disease in the metropolis. The commission examined Power’s evidence, and other information from Stockwell, Homerton, and Datcham which confirmed the risk of living near a smallpox hospital.11 It recommended that cases in future should be transported by river to hospitals situated on the banks of the Thames and that only those too ill to be moved should be treated in the metropolis. For the severely ill, small 30-40 bed units should be provided in the fever hospitals and used only for patients from the immediate neighbourhood. Sensitive to the opinion of local residents about the value of their property, the Metropolitan Asylums Board renamed its hospitals, using postal divisions instead of the older names of Hampstead, Fuiham, Homerton and Deptford.9 Under the chairmanship of Sir Edmund Hay Currie, the Metropolitan Asylums Board adopted the new policy ‘in a manner which did them credit’. Throughout 1884-5 architects were hard at work designing wharves for Fulham, Poplar* and Rotherhithe.12 Ambulance steamers were built and a series of floating and riverside hospitals were established so that patients could be sent down river for treatment. [Managers Street, Poplar, was built to connect the main road to North Wharf, and existed until the redevelopment of Docklands]. The epidemics of 1881 and 188413,14 confirmed that smallpox spread from hospitals. In 1886 the Metropolitan Asylums Board decided that it would no longer receive smallpox cases in hospitals within the urban areas.8 Nevertheless for financial reasons the Local Government Board was slow to agree to the construction of a convalescent hospital at Darenth for 600 patients. The old Highgate Smallpox Hospital building was sold to the local guardians and the hospital moved to Clare Hall, South Mimms. The debate continued about the route of communication of smallpox - whether it was by aerial infection or direct person to person contact. A report to the Local Government Board in 1894 pointed out that even when the Metropolitan Asylums Board had tightened all its regulations and communication with the outside world was at a minimum, smallpox inexplicably appeared in nearby houses when cases were admitted to the Fulham hospital.8 Once the policy of riverside hospitals was adopted the problem ceased. The managers of the board, with their excellent ambulance and ambulance steamer system, telephonic communication and disciplined staff, had found the solution. The poor of London showed an increasing tendency to seek hospital treatment. The annual reports of the Local Government Board demonstrated that fewer and fewer were dying of smallpox in their own homes:
The original smallpox hospitals had been of moderate size. It became necessary to provide for larger numbers of patients and the Poor Law Act of 1889 further increased the demand for accommodation by making admission possible without the stigma of becoming a pauper. The new fever and smallpox hospitals which were built on the periphery of London were larger as well as being further from the centre. The willingness of the Metropolitan Asylums Board to act on the best professional advice available, and the efficiency of the ambulance and hospital services it provided, were the foundation of the respect and reputation that the board enjoyed. It might be chided for the grand scale of its expenditure, but The Lancet said that it provided, if not a perfect system of isolation accommodation, the nearest approach to a perfect system which the world possessed.15 Its administrative staff earned a reputation for competence, and were regarded as a cut above those employed by the guardians. ‘They were up to LCC standard’ said one county council man. As a result the remit of the board was gradually extended. From the beginning it had a responsibility for ‘harmless insane paupers of the chronic or imbecile class’ and later it treated conditions which might have been cared for in hospitals or infirmaries. In time it came to provide services for venereal disease, encephalitis lethargica, tuberculosis and uterine cancer. In part it became a general hospital authority, albeit one which worked under the Poor Law.
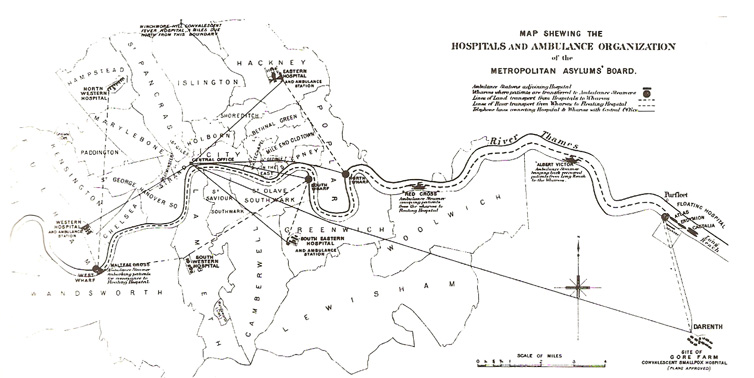
Map showing the hospitals and ambulance organisation of the Metropolitan Asylums Board, source: Burdett HC. Hospitals and Asylums of the World 1893 Material about workhouses and smallpox and fever hospitals is on-line at www.workhouses.org. 1 Ashley Chadwick E and Southwood Smith T. Report to the General Board of Health on epidemic cholera. London, HMSO, 1850. 2 Highmore A. The history, design and present state of the public charities in and near London. London, Cradock, 1814. 3 The London Fever Hospital. Lancet, 1848, ii, p 483. 4 House of Commons. Select committee on Hampstead Fever and Smallpox Hospital. London, 1875; and Lancet, 1875, ii, p 180. 5 New Hampstead fever hospital. British Medical Journal, 1870, i, p 142. 6 The Hampstead hospital question. Sanitary Record, 1874, p 452. 7 The new ambulance station of the Metropolitan Asylums Board. British Medical Journal, 1881, ii, p 567. 8 Thorne T. Memorandum on smallpox hospitals by the medical officer. London, Local Government Board, 1894. 9 The aerial diffusion of smallpox. Lancet, 1883, ii, p 997. 10 Local Government Board. Supplement to the tenth annual report on the use and influence of smallpox hospitals. London, HMSO, 1882. 11 Power W H. Report on the influence of the Fulham Smallpox Hospital on the neighbourhood. Appendix M. Hospitals Commission, 1882; and Report and evidence to the Hospitals Commission on the Smallpox and Fever Hospitals of London. London, HMSO, 1882. 12 PRO/MI-L/14/22. 13 Hampstead and Highgate Smallpox Hospitals. Lancet, 1886, i, pp 310, 360, 1031; and British Medical Journal, 1886, i, p 263. 14 The metropolitan smallpox hospitals. British Medical Journal, 1886, i, pp 361, 707. 15 The Metropolitan Asylums Board in 1895. Lancet, 1896, ii, p 1029. Further reading Ayres G M. England’s first state hospitals and the Metropolitan Asylums Board. London, Wellcome Institute of the History of Medicine, 1971. The Metropolitan Asylums Board. London, Metropolitan Asylums Board, 1931. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
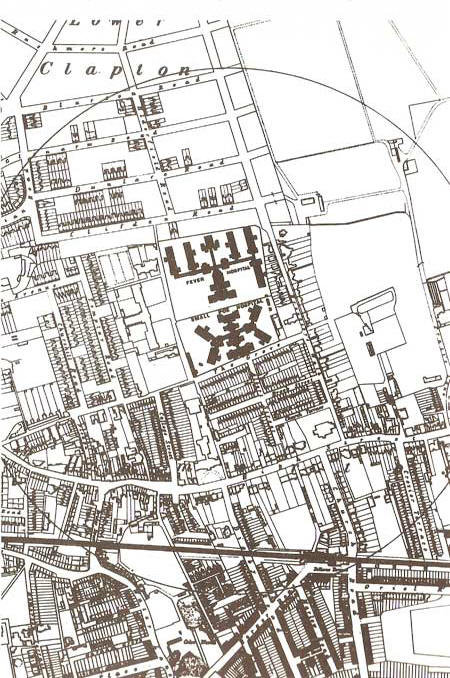 Map
showing the Homerton (fever) Hospital, source Hospitals Commission 1882
Map
showing the Homerton (fever) Hospital, source Hospitals Commission 1882