Reviewing the past and shaping
the future
‘London has hitherto been the despair alike of statesmen, politicians and philanthropists. Its political apathy no less than the appalling mass of squalid destitution it contains is a positive danger to the commonwealth.’1
Sidney Webb, The London Programme, 1891
|
The vast improvement in care since the middle of the century as a
result of anaesthesia, antisepsis and the introduction of trained
nurses increased the numbers seeking hospital care and was
associated with a reduction in the time patients stayed in hospital
and an increased admission rate. Developments in hospital
administration were less impressive. As a result there was a series
of wide-ranging reviews in the twenty five years preceding the Great
War. Twenty years of academic dispute and debate culminated in the restructuring of the University of London to permit the University both to examine and to teach. Sidney and Beatrice Webb, and the Liberal politician R B Haldane, were prime movers in this, but the measure was so far from satisfactory that a Royal Commission was established to re-examine the question within a few years. Finally, against the background of changing social and political attitudes, the principles of the Poor Law were re-examined by the Royal Commission of 1909. The Charity Organisation Society and the enquiry into the hospitals Since the l850s, dissatisfaction with hospital management had been growing. Continuous lobbying by the Charity Organisation Society eventually obtained an enquiry. It also ensured that the society would maintain an influence over the proceedings2 The society had established a special committee on the reform of the metropolitan medical charities which met weekly from the end of 1888. Timothy Holmes of St George’s was invited to join and agreed to do so, although he said that he did not expect to receive much support from the medical profession at large. Ernest Hart, editor of the British Medical Journal, offered its support. The committee collected detailed information, sought the support of men of eminence, selected potential witnesses and, after taking soundings, drew up a petition seeking the appointment of a commission. In January 1889 the society’s secretary, Charles Loch, was instructed to write to the press to ask those who were interested to contact him. Neither Sir James Paget nor Henry Burdett favoured an enquiry but many others did, including Sir Sydney Waterlow, treasurer of St Bartholomew’s, and Sir Spencer Wells. Henry Burdett wrote in The Hospital that what was really needed was a short Act of Parliament which would prevent a hospital being opened unless there was a need for it, that the bona fides of its protagonists were beyond question and that funds were available to support the new institution.4 In April 1889 the petition was widely circulated to hospital governors, doctors, boards of guardians and the newly formed London County Council. An editorial in the British Medical Journal welcomed the move and in particular the chance to examine the relationship between voluntary charity and poor law medical relief.5 There was considerable discussion within the special committee about who should present the petition to the Lords and several members of the upper chamber were approached without success. Lord Sandhurst, the chairman of the Middlesex Hospital and himself a leading member of the special committee, ultimately did so. On 29 July 1889 he addressed the Lords and presented the petition, now signed by many members of the medical profession including Sir John Simon and Sir Spencer Wells and eminent laymen on behalf of various charitable organisations. In his speech Lord Sandhurst outlined the size and expenditure of the voluntary hospitals and infirmaries, criticising the special hospitals in particular. He said that the origin and management of many of them were suspect, and implied that they were started for the private advantage of those who wished to make themselves consulting physicians, or purely for speculative reasons. The Society’s petition was in fact a plea for an enquiry into the possibility of organisation in medical charity, but it was seen as its usual type of attack upon the hospitals. The Hospitals Association, whose members were working hard to improve matters from within, were not enthusiastic about an enquiry. The British Medical Association, as Hart had promised, welcomed the Charity Organisation Society’s proposal for an enquiry at its annual meeting. Indeed many branches of the Association wished it to be extended to cover the entire country, a proposal which was resisted by the London committee of the Charity Organisation Society.6 While the Government was considering its response, the special committee drafted the evidence to be given to an enquiry by its secretary. Lord Sandhurst suggested that it should be prepared to produce some scheme for the better management of the metropolitan medical charities. He also discussed matters with ministers. By March 1890 the Charity Organisation Society had drafted and agreed proposals for improving the administration of the medical charities. At first sight the welfare of the hospitals was not a party matter, but the great hospitals were particularly sensitive about the possibility that a royal commission would be established. Lord Cranbrook, the minister responsible, decided instead upon a select committee of the House of Lords. On 28 April 1890 a motion in the House established a select committee, to be chaired by Lord Sandhurst himself. It was agreed that the remit of the select committee would be: ‘to enquire with regard to all hospitals and provident and other public dispensaries and charitable institutions within the metropolitan area for the care and treatment of the sick poor which possess real property or invested personal property, in the nature of endowment, of a permanent or temporary nature; and to receive, if the Committee think fit, evidence tendered by the authorities of voluntary institutions for like purposes, or with their consent, in relation to such institutions: and further, to inquire and report what amount of accommodation for the sick is provided by rate, and as to the management thereof.’7 The establishment of the select committee was a victory for the Charity Organisation Society and those of like mind. However others were apprehensive. Burdett said that the pressure for reform came from ‘disaffected persons with axes to grind’ and was not in all respects altruistic. One of the chief axe-grinders was Dr Robert Rentoul, a Liverpool general practitioner with British Medical Association affiliations, who published a book on voluntary medical charities whilst the Lords’ committee was sitting.8 Rentoul said that four groups were bringing discredit to the hospitals — hospital committees who would ‘sell charity’ in the form of letters of recommendation to anyone willing to purchase them, well-to-do workers who would accept charity as a right, those who bought governors’ letters and tickets of recommendation to provide cheap care for relatives, friends and employees, and doctors who used the charities for the purpose of self-advertisement. Another undercurrent was the campaign for a national register for nurses, led by the British Nurses’ Association. Partisan conflicts emerged in the evidence given to the committee, and heralded the thirty year ‘battle of the nurses’. Against registration were most hospital governors and doctors, the matrons of many of the large hospitals like the young and energetic Miss Lückes of The London, Miss Monk of King’s and Miss Nightingale herself. ‘Twenty or thirty years hence, when progress has been made’, said Miss Nightingale, ‘this registration might do’.9 Other opponents included the majority of those actively involved in training, who pointed out that training had only existed for a couple of decades, and properly trained nurses were in a minority. The profession was in a state of transition. There was a fear that an ‘unrepresentative organisation would enforce a uniformity of theoretical knowledge which would be contentious and would leave out the qualities of gentleness, quick observation and quiet self-control which could not be assessed by examination’.10 Miss Lückes believed that registration would injure the status of the ‘well-trained nurse’ by making it hard to distinguish between those with first-rate and those with second-rate qualifications. Nearly all metropolitan hospitals and very many large provincial hospitals had much to lose and nothing to gain by levelling down standards. She thought that the qualities of a nurse could only be assessed by her training institution, and that a register would give a false sense of security.10 On the other side were many of the younger nurses who wished for professional advancement and relief from autocratic rule. They were led by Mrs Bedford Fenwick, the ex-matron of St Bartholomew’s, and editor of the Nursing Record. She campaigned for a three-year training, like the course she had introduced at St Bartholomew’s, with an objective assessment of the competence and knowledge of nurses. The Lords’ committee came to spend much time on a series of accusations against the matron and the nursing regime of The London Hospital, some of which reflected personal animosities. Members of the Charity Organisation Society committee expressed regrets that more attention which was paid to the internal affairs of a single hospital merely diverted the select committee from matters of greater importance.3 The evidence of the Charity Organisation Society The Lords’ committee had received a mandate to examine and report upon problems which had been of concern for many years. Lieutenant-Colonel Montefiore, who was the first witness and the secretary to the special committee of the Charity Organisation Society, gave his evidence with force but moderation. He said that his Society existed to improve the condition of the poor by propagating sound principles of administration, promoting the cooperation of charities, discussing practical questions, working for reform when necessary and promoting thrift and self-dependence. Speaking from a carefully prepared brief he was at pains to stress that the Society was not hostile to the hospitals which were ‘glorious institutions’ nor did it wish them to be rate-supported. But improvements could be suggested.11 The Society was concerned about poor conditions in outpatient departments and their use by patients who were not entitled to charitable relief. The charitable organisations had little contact with each other and in any case free treatment was of little use to those without food and the comforts necessary to health. Most hospitals were in the centre of town and those living further out had no local service and a long distance to travel. Doctors in poorer areas had difficulty in making a living because of the many charitable and part-payment services. The continuous competition between hospitals, both for patients and to increase their services, drove them to all manner of contrivances to meet the debts they incurred. New hospitals were being established without reference to the need for them. The Society made constructive suggestions to remedy these defects. It believed that the infirmaries should be brought into closer relationship with the hospitals, and joint medical staffing should be encouraged. It envisaged a supervising council which would report either to the Charities Commission, the Local Government Board or the new London County Council. This would be formed from the chief professional, hospital and charitable interests and would be similar in composition to the Assistance Publique in Paris. It would arrange for visitors to inspect the hospitals and suggest necessary improvements. The supervising council would publish an annual report on the finance and management of London hospitals, reporting the action taken to achieve coordination and the suggestions it had made which hospitals had ignored. It would supervise the development of hospitals and the establishment of new medical charities; receive funds and legacies; and not only distribute money in its own right but advise the organised charities on the allocations they made. The slow progress which had been made by the Sunday Fund suggested that its composition and policies were not suitable for the task in hand. The council would need to reduce the load on outpatient departments, to improve the quality of patient care and encourage the use of poor law infirmaries for teaching. It would seek economy of administration, uniformity of accounts and rationality in the establishment of new hospitals in order to develop a system of districts, each with its own hospitals. Faced with such proposals the Lords quickly went beyond their financially oriented terms of reference. Witness after witness was asked to give evidence and the press recognised the care with which the select committee went about its task and the fundamental issues which it was exploring. Here would clearly be a document of stature, for the witnesses came from widely divergent backgrounds covering the entire spectrum of professional and administrative opinion. Yet the Charity Organisation Society influence remained powerful. The society designed and printed the questionnaire which was sent out to all the hospitals by the select committee and later analysed and arranged the printing of the replies. It prepared a map of the London hospitals for the committee and kept in close touch with its chairman. Charles Loch was instructed to list and contact the younger men on the medical staff of the hospitals.3 He did so, but reported that little would be gained from them and that they showed ‘a want of knowledge on the Hospital question’. The committee sat for two years and produced a four volume report. The evidence of the witnesses provides a wealth of information about the conflicting attitudes and the conditions of medical practice in London at the end of the nineteenth century (see Tables 10 and 11, page 139) The last witness was Charles Loch, who reiterated the views of the Charity Organisation Society and summed up the case for change.” The report of the select committee The final report was published in 1892 and appeared to be a vindication of the voluntary system for it stated that in general the hospitals were well administered, though in the endowed hospitals too much power and responsibility often rested upon one man — the treasurer. This accusation was not new. Others saw the report as opening the door to sweeping reforms. The committee urged the need for coordination of the general and special hospitals and the poor law infirmaries: ‘...so far from there being at the present time any general system of combination or any definite division of work among the various institutions they are on the contrary for the most part competing with one another at every point for public support, and to a great extent for patients. This condition of things is wasteful and prejudicial to the sick for whom these institutions exist and to the interests of medical science and education. The evils of the present system, or want of system, are generally admitted but little has been done hitherto to cure them. Much improvement might be affected by affiliating special hospitals to general hospitals but next to nothing seems to have been done. A scheme was proposed for dividing the whole of London into districts, each district to be supplied within its own limits with the necessary provision of hospitals.’ The twelve general hospitals with medical schools in 1889
Source: Report of the Lords’ Committee, 1892. Their Lordships commented on the congestion of hospitals on the north side of the Thames and reported that ‘the prevailing though not unanimous opinion seems to be that on the whole hospital accommodation in London is sufficient; but much inconvenience and a partial inability in some places to cope with demand for admission are caused by unequal distribution and want of organisation’. Some witnesses thought the difficulty might be met by transplanting some of the hospitals in the central district to places in the north, south and east where they are more wanted. They recommended the establishment of a large general hospital in densely populated Camberwell, if a site could be found and the money could be raised. Distribution of London hospitals in 1890
source: statistics prepared by H C Burdett The use of poor law infirmaries for educational purposes was advocated. The committee stated that ‘the infirmaries afford a field for the study of precisely those chronic and intermittent cases which the young doctor will most frequently meet when he goes out into private practice and which he has the least opportunity of studying in the wards of the general hospital, where all cases are severe and acute. Just as the outpatient shows to the student the beginnings of disease, so in the Poor Law Infirmaries he ought to watch its continuing and closing phases.’ The committee heard conflicting views on the role of outpatient departments, but concluded that they were necessary, if only for educational purposes. However the number of patients seen each day should be restricted, and the use of departments for consultative purposes should be encouraged. The question of a nurses’ register went to a vote; Lord Sandhurst was in favour but he was outvoted and no recommendations were made. The committee recommended that the University of London should be enabled to teach medicine as well as to examine, and that the medical schools should be affiliated to the University. The report received a favourable reception and it was summarised in the medical press. Burdett discussed the findings in the introduction to volume three of Hospitals and Asylums of the World, which appeared in 1893. The worst fears had proved groundless. Each group fastened on the recommendations most to its liking, although the British Medical Journal accused their Lordships of being far from thorough in their consideration of abuse of the outpatient departments, dismissing the accusation in a light and airy way.12 The special committee of the Charity Organisation Society ceased to meet. It had finished its work. Charles Loch wrote in The Nineteenth Century about the need for action.13 Mouat wrote four articles in The Lancet saying that he hoped that a central board would be formed with all the power over the general hospitals that the Metropolitan Asylums Board had over fever hospitals. He repeated his proposals for five districts based upon the registrar general’s five districts. The attempt to establish a central board The Lords committee had agreed with the Charity Organisation Society that there should be a central board. This would act as a watch-dog, audit accounts, describe operational policies, publish and comment upon proposals to remove, expand or open hospitals, and act as a central charity for the receipt and distribution of endowments and contributions. The board’s power would be limited and it would not interfere with local management; neither would it receive a government grant for this would reduce the flow of voluntary contributions. Nevertheless the Lords believed that people would heed a board’s comments on proposals to build ‘useless hospitals’, and on the quality of a hospital’s administration. A central board would help in times of financial difficulty, the Lords fearing that without one the time would come when voluntary hospitals would need government or municipal aid. Sidney Webb, in The London Programme which was prepared with London County Council elections in mind, also thought that a separately elected Board was desirable. But he saw a Board as a first step to the replacement of private hospitals by public institutions. ‘London’, he said, ‘must systematically undertake the care of London’s sick.’1 The chairman of the select committee, Lord Sandhurst, did not consider his work complete with the publication of the report. Wishing to oversee its implementation he invited representatives of the central funds and the hospitals to a conference at Spencer House in July 1892, to consider the formation of a central board. The invitation gave rise to much discussion in hospital circles for while many were opposed to cooperation there was little desire to offend the noble Lord. Burdett, who was invited to the conference, noted ‘a want of genuine interest in the proposals, much doubt as to the practicability of devising a scheme for cooperation, and an undercurrent of desire to do nothing.’ He predicted that a committee formed by the conference to consider how a board might be established would have a ‘thorny path to traverse’. He wrote in The Hospital that a central board without the power of the purse or the authority to enforce its recommendations would probably accomplish little, whilst its power for evil might be considerable.15, 16 A proposed pattern of membership was rejected by the hospitals as biased towards the medical charities and unrepresentative of the voluntary system. The opponents of a board included many who objected to centralism in all its forms. They feared an infringement of the rights of hospitals to continue to act as separate units, and wished to preserve absolute individual freedom. Nevertheless Louisa Twining, a veteran campaigner, said that she was convinced that there was something in the hospital system which could be made more in accordance with modern needs and modern ideas.17 Regular meetings were organised by the Charity Organisation Society and in January 1897 its secretary outlined the principles he believed to be generally accepted i Any board should be representative of the main interest groups. ii Reliance should be placed upon cooperation and publicity rather than on legal measures and compulsion. iii A central fund should be formed as a permanent endowment of the hospitals. Opponents of a central board were given the chance to make their case at a meeting called to consider the proposition, but as those present were largely the protagonists the vote in favour of a board was 121 to 12. The view of the majority was that a board was necessary to maintain the health of the voluntary system, and it was the only way to ensure that London’s hospital and medical needs were considered as a whole.18 The Society established a sub-committee to produce a new scheme giving the hospitals the increased representation they demanded. Each hospital would have direct representation, with additional seats for the central medical charities and general practitioners. The result was a board so big that an executive committee would also be necessary. Deputations to the hospitals received little encouragement. Few hospital representatives turned up at the meeting convened to consider the scheme. A central board with two hundred members seemed so impracticable that they were not prepared to spend time discussing it. Those seeking autonomy for the hospitals believed that if a board controlled funds it would be dangerous, and if it did not it would be useless. Instead, the twelve hospitals with medical schools met separately at the Westminster Hospital and formed a Central Hospital Council for London, to consider matters in which they had a common interest and promote joint action.19 The Hospital Reform Association Much of the pressure for a central board came from the general practitioners. The Hospital Reform Association, formed in 1896 ‘to concentrate medical opinion on reforming hospital administration’, was largely a general practitioner body. The president had been president of the British Medical Association. The British Medical Journal was an ally, and those favouring provident dispensaries like Timothy Holmes and Charles Loch were members. The Association set to work, organised conferences, and prepared a report on the management and financial arrangements of the special hospitals, demonstrating how much of their income came from payment bypatients who did not require charity. The special hospitals were not even keeping to their own specialty. The Cancer Hospital was treating piles, fistulae, tuberculosis and syphilis, and the Chest Hospital anaemia and Lord Lister, in a private letter, described the Association as ‘a most unwieldy and heterogeneous body in which the medical profession was chiefly represented by practitioners whose names carried little or no weight and whose outcry against hospital abuse was extremely exaggerated’.21 He was not alone in this opinion. Sydney Holland (later Lord Knutsford), the chairman of The London Hospital, also disapproved of it, saying that the Association was chiefly got up by some gentlemen from Wales. The reformers came to see that they could expect little support from the hospitals. Few of the hospitals’ medical staff wished to restrict the flow of patients. Hospital administrators saw no advantage to the reputation of their hospitals or their funds from turning away patients. The Royal College of Physicians declined to take any initiative. The Charity Organisation Society had more success in achieving the introduction of a system of enquiry into the means of patients in outpatient departments. In 1895 an experienced Charity Organisation Society district secretary was appointed at the Royal Free Hospital, her salary being paid by the society for the first three months. Miss Stewart, the first of the lady almoners, was followed by others trained by the society. Soon almoners were appointed at St Bartholomew’s, The London and the Hospital for Sick Children. Some society members, also members of the council of the Sunday Fund, encouraged that Fund to regard the appointment of almoners as a ‘merit’ to be taken into account when money was distributed. The job of an almoner was not an easy one. They were faced by crowded departments seeing thousands of patients a year. The secretary of The London Hospital pointed out that the cost of employing an enquiry officer itself reduced the funds available for relieving the sick poor.22, 23 The LCC and the Metropolitan Asylums Board The quest for better methods of organisation was not restricted to voluntary hospitals. In 1893 the newly established London County Council asked a sub-committee to consider the overlapping activities of a number of centralised rate-supported bodies in the fields of health and education. The sub-committee’s report was considered by the Council in June 1894. It dealt with the wide range of services provided by the Metropolitan Asylums Board, which by now included fevers, infectious diseases, the mentally handicapped and even groups like pauper children who were sent to training ships. The Hospital Commission on smallpox in its 1882 report, had recommended that responsibility for the sanitary state of an area should be in the same hands as the management of hospitals for fevers. The London County Council, debating its subcommittee’s report, came to the same conclusion. The Council, of which Sidney Webb was a member, adopted the policy that all central metropolitan powers in the field of public health should be in the hands of ‘the elected representatives of the rate-payers’, and that the services provided by the Metropolitan Asylums Board should be transferred to the Council. The Lancet thought this proposal was ‘absolutely sound’.24 Before the formation of the London County Council The Lancet had thought that the Metropolitan Asylums Board had the potential to become the central heath authority for London. Now that the Council was establishing a firm claim to this role it would inevitably become, sooner or later, the manager of the services provided by the Board.25 The Prince of Wales’ Hospital Fund for London [The Fund did not adopt its present name until the death of Queen Victoria] Few of those who have devoted their lives to London’s hospitals can have accomplished more than Henry Burdett. Because of his long established position in the hospital world he had been associated with LordSandhurst’s attempts to form a central board, of which he did not altogether approve. In 1896 he was at the centre of discussions which bore more lasting fruit.
Throughout his life he was careful
never to claim that he had played a key role in the foundation
of the Prince’s Fund. As one of the Prince’s trusted
advisers he may have believed that more is accomplished if one
does not insist on claiming the credit. However many of the
characteristics of the Fund bore Burdett’s stamp upon them, and
reflected ideas he had advanced many years before. From his early years the Prince had been interested in hospital affairs. He had accepted the presidency of St Bartholomew’s as early as 1867 and he regularly undertook to open new hospital buildings. He became patron of The Hospital Saturday Fund in 1896, and The Lancet said that scarcely a week passed without his making an effort for the public good. His interest and example ‘might be the very saving of the voluntary hospital system’. Help was certainly needed, for in 1894 the Hospital Sunday Fund said that around £300,OOO was vital to cover the liabilities of the London hospitals and dispensaries. It had taken 20 years for the Sunday Fund collections to rise from £27,000 to £40,000 a year, and an appeal by University College Hospital in 1896 produced so derisory a sum that the governors were forced to comment on the lamentable indifference in the district to a charity of vast importance to the poor of the neighbourhood. Another 50 beds were added to those already closed in London.26 In 1896 the governors of Guy’s decided to launch an appeal to ‘reendow’ the hospital and reopen beds which had been closed. Presiding at the festival dinner, the Prince thanked Henry Burdett for his efforts in the hospitals’ cause, and for his work as a steward to make the dinner a success. It was Burdett who first suggested the idea of a fund to the Prince, who initially questioned the leadership of such an appeal by a member of the royal family, and the association of the fund with Queen Victoria’s Diamond Jubilee. The risk of rivalry with Hospital Sunday arose, but at length agreement was reached.27 Even before Jubilee year began rumours were circulating about the possibility of a commemorative fund. The Lancet expressed the hope that a group of wise and influential people might invite contributions, and that the money might go to the hospitals rather than to a district nursing fund as on the occasion of the Golden Jubilee.28 By 16 January 1897 the name of the Prince was being coupled with the possibility of a hospital appeal. The rumours intensified when Sir William Broadbent addressed the Charity Organisation Society, mentioning the possibility of a gigantic scheme for collecting money for the benefit of the hospitals on behalf of the Prince of Wales. Gigantic it would be, for if its object was to provide the additional £100,000 a year the hospitals needed, either from annual subscriptions or as income from investments, the effort required would be enormous. Sir William pointed out the need for a distribution committee to obtain information from the hospitals and to allocate money on the basis of their merits. The Lancet thought that the committee established by the Charity Organisation Society to work for the formation of a central board could serve the Prince well. The Charity Organisation Society had never shown much of a tendency to help the hospitals with their financial problems, although it was ever ready with good advice. Now was the time for all to work together for the good of the hospitals.29 The accuracy of the rumours became apparent when the Prince wrote to the press to launch the appeal. Those invited to the first meeting of the general committee on 21 January 1897 at Marlborough House were mainly of high rank in the church, the City or the state. Burdett was present, and he became a member of the Organisation Committee formed in February 1897, which met two or three times a week to get the appeal under way.30 Burdett was a member from the outset of every significant committee formed by the Fund, and it was said that in twenty years he never missed a council meeting. He personally undertook much of the early correspondence with the press, the savings banks and the printers, and he assisted in the selection of the first permanent officers.31 For these services he was awarded the KCB in June 1897.27
Introducing the
appeal the Prince said: ‘Public opinion has shown itself on more
than one occasion, and I think wisely, in favour of the
voluntary system for support for our hospitals, combined with an adequate system
of representation of the body of subscribers in their control
and management. It is obvious, however, that if these
institutions are to be saved from state or parochial aid, their
financial condition must be secured.’ The aim of the Fund was to
place them on a sound financial footing with an additional
assured income of £100,000 a year.32 The
Prince himself took the lead in selecting the members of the
general council, chairing its meetings. Lord Rothschild agreed
to become treasurer, and wrote to city financial institutions
seeking donations. The Lord Mayor of London pledged his support,
Grocers’ Hall and the Bank of England provided premises and
facilities, and two conferences of the clergy supported the
appeal. Unlike the councils of the Sunday and Saturday Funds,
whose members were essentially representatives of the
subscribers and subscribing bodies, members of the council of
the Prince’s Fund were personally selected. To be appointed to
the council was a high honour and feelings might be hu Hospital stamps were printed by De la Rue for sale to allow all class to subscribe with the minimum of difficulty; it was Burdett's idea. The plates from which the stamps were printed were smashed ceremonially when the run was completed. Each stamp bore the Prince’s signature and a picture of Charity, after a painting by Sir Joshua Reynolds. The 1/- stamp was blue, the 2/6 orange, and they could be stuck in a small book which contained a message from the Prince. A second issue of charity stamps the following year was less successful, and this method of raising money was abandoned. The development of the Fund’s policies There was widespread acceptance of the Prince’s view that state control of the hospitals should be avoided. Even the radical and reforming Lancet had ceased to advocate the establishment of state hospitals, believing that patients were cared for better under a charitable system, that the management of individual hospitals was better than ‘local municipal wisdom’ and that state control would lead to the loss of charitable money.33 The council of the Prince’s Fund appreciated at an early stage that the great difficulty would be who was to administer the fund. If a board was constituted, the great hospitals, and probably the lesser ones as well, would claim representation on it.34 The Fund received much free advice. The secretary of the Royal Westminster Ophthalmic Hospital suggested that the Coal, Corn and Finance Committee of the Corporation of London would distribute the money sensibly. C S Loch wrote to The Times to urge the Fund not to use the method adopted by Hospital Sunday, which had showed little inclination to use its power to stamp out hospital abuse. The Lancet wanted the Prince to limit the duration of his appeal to avoid undermining the existing central funds. Distributions should also be made in a way which would discourage abuse by those above the poverty line, doctors should have a say in the way the money was distributed, and the opportunity should be taken to initiate a central board. The British Medical Association believed that monies as vast as those of Hospital Sunday and the Prince’s Fund should be distributed by a committee which worked in public, including representatives of the hospitals themselves, akin to the central board for which the Charity Organisation Society was pressing. It would then become the parliament of hospital finance in London.35 36 The views of Stephen Coleridge, treasurer of the Victoria Street Society for the Prevention of Vivisection, were predictable. In a letter to the Prince, released to the press, he asked that hospitals whose medical schools conducted experiments on ‘helpless dumb animals’ should be excluded from the distributions. On 8 May 1897 Sir Francis Knollys replied in His Royal Highness’ name that there was no intention of devoting any part of the Fund towards the support of medical laboratories.37 The Prince decided that the appeal should not be limited in its duration but to avoid trespassing on the sources of money of the Hospital Sunday and Saturday Funds appeals would not be made from the pulpit or in factories. Many feared that money given to the new fund would merely be diverted from the other central funds, or from the hospitals themselves. Because of the controversial nature of the Charity Organisation Society’s proposal to establish a central hospital board, to which the hospitals were opposed, the Prince’s Fund decided that it would be inexpedient to be associated with that movement, or with the Hospital Reform Association.30The Lancet came to believe that this was a sensible decision, for even the protagonists of the idea could not agree on the form a board should take. As soon as the appeal had been announced letters began arriving; some enclosed donations, small and large, others asked for assistance. The Mayor of West Ham wrote saying that his borough was really part of London; he would launch a local appeal for the Fund if he was assured that West Ham’s hospitals would be eligible for a grant. Less subtle correspondents, like some from Finsbury, were told that it was too soon to enter into questions of distribution. Allocating the money Amongst the Prince’s advisers was Lord Lister, who was asked to give his views on the way the money should be distributed. Lister thought that while examining the management and financial needs of the hospitals would be a considerable task, the greater problem would be to decide which hospitals were run on a sound professional basis; poor decisions would bring the Fund into disrepute. An authoritative group of advisers was necessary and Lister thought that the Central Hospital Council, formed by the teaching hospitals after the outcry against ‘hospital abuse’, would serve the purpose. Its chairman, Sir Trevor Lawrence, agreed it should assist if asked.38 To turn to outside bodies for advice was not what the Prince had in mind. Following a memorandum on methods of allocation written by Burdett30, a distribution committee was formed which in turn appointed a visiting committee to inspect the hospitals. The visiting committee consisted of physicians and surgeons of wide experience, with an equal number of laymen who were interested in hospital management. In the first year the Fund sought the assistance of Hospital Sunday, and in June 1898 asked the advice of the Central Hospital Council on the management of certain small and special hospitals. After that it relied entirely on the advice of its distribution committee, chaired by Lord Lister, and the visiting committee under Sir Trevor Lawrence. Hospitals lying within seven miles of Charing Cross were divided into four groups: north-west, north-east, south-east and south-west, and underwent ‘thorough inspection and enquiry’. The report on The London Hospital showed that much needed to be done, and it was agreed that if the hospital would spend up to £100,000 of its own capital on the necessary work, the Fund would make an annual grant of £5,000 — well above the level any other hospital received. Money was usually distributed for specific purposes, to open closed beds and to improve facilities, as well as a general grant-in-aid. The Prince wished capital sums to be allowed to accrue, only the income being distributed. The distribution committee was therefore able to provide more support year by year, and annual grants were reasonably secure. While the Sunday Fund’s grants were used for general maintenance, those of the Prince of Wales’ Fund were an instrument of change, strengthening the hospitals and the voluntary system. Hospitals were given a clear idea of what was expected of them, but the visitors’ remarks were confidential as the Fund did not wish them used as evidence of need when an appeal was to be launched. Grants were in danger if the next report from the visitors indicated that no action had been taken. It became Fund policy to make grants of considerable size for major schemes of great importance. Guy’s asked for assistance in the reconstruction of its outpatient department, and St Bartholomew’s itself sought a contribution to its rebuilding fund. Sir Savile Crossley, speaking about the new Fund, said that its work ‘as an intelligence department, obtaining and collating information and statistics relating to the hospitals, was of the first importance’. By degrees the examination of figures which had been verified by visits would enable the Fund to form useful opinions on many questions relating to hospital management. There was hope that this would be a means of preventing many of the mistakes and extravagances of the past.39 From an early date the Fund made it clear that hospitals receiving grants were expected to maintain high standards of efficiency in organisation and equipment, and it was soon involved in advising hospitals on financial and architectural aspects of building schemes. Plans were sent to the Fund for comment in the hope that a capital contribution would accompany approval. When the annual accounts were submitted, the Fund would draw attention to above average expenditure. A patient’s complaint or a press report which painted a voluntary hospital in a bad light would lead the Fund to ask the chairman of the hospital concerned for comments. After Queen Victoria died the Fund became known as King Edward’s Hospital Fund for London. The new Prince of Wales assumed the presidency but King Edward VII remained the patron, and donated the money which had been collected as his coronation gift. Further endowments in 1902 from Lord Mount-Stephen and Lord Strathcona brought the Fund to within striking distance of its target income of £100,000 a year. Regrettably by this time few still believed that even a sum of this size could keep London’s hospitals solvent. In 1907 the Fund received a charter, under a private Act of Parliament, which established the constitution and governance. The royal presidents remained active in its affairs, approving minutes and expressing views on matters of significance. From the start the Fund was not merely a source of money but of good advice. The Central Hospital Council for London The Central Hospital Council, formed in November 1897 to defend the interests of the teaching hospitals, consisted of representatives of the management bodies and medical staffs, but proved to be ineffective and unable to influence events. It did not have the resources of the King’s Fund, nor did it always command the support of its constituent members. It fought for a reduction in hospital rates (1898), considered ‘hospital abuse’ (1899) and discussed the anti-vivisection campaign (1900). It opposed the creation of a central bed bureau when the Hospitals Association proposed one, as inexpedient and lacking ‘practical utility’ (1903). It opposed state registration of nurses (1904), and considered the charter of the King’s Fund unsatisfactory (1907). It gave evidence to the Royal Commission on the Poor Laws (1908) and commented on the National Insurance Bill (1911). However the hospitals took little interest in its work, and the chairman, Mr Harben of St Mary’s, resigned in 1910 because the council seldom gave a lead, preferring to delay discussion until the hospitals had already decided what should be done. Harben said that the council tended to shrink from the questions addressed to it, and he doubted if it could serve any useful purpose. Indeed major problems like the question of hospital relocation and rebuilding were not considered at all by the council. Nevertheless it continued to meet until the 1914—1918 war.19 Because the London medical schools were essentially part of their parent hospitals the financial arrangements between school and hospital were close and complex. For example at the Middlesex the school had been incorporated into the hospital in 1895, and placed under the management of a council of lay governors, medical staff and medical school teachers. At Guy’s, Herbert Eason the dean wrote in 1904 that the medical school had no corporate existence and no property. Out of the students’ fees a fund was formed, but without doubt this belonged to the governors.41 Stephen Coleridge, Hon Secretary of the Victoria Street Society, became interested in the schools’ accounts and their sources of income. He examined the accounts of Guy’s in 1897, and it is probably significant that when the Prince of Wales opened the hospital’s new medical school laboratory that year he said that the experiments conducted on animals were performed under anaesthetic and in the interests of suffering humanity. In May and June 1901 Stephen Coleridge and the British Medical Journal disputed whether teaching hospitals like Guy’s, the Middlesex, The London and Charing Cross, which had received sizeable grants from the King’s Fund, had thus been enabled to increase the sum they made over to their schools. Coleridge believed that contributors to hospital charities did not wish their money to be spent on animal experimentation. He raised the question of ‘the appropriation by the medical schools of money raised for other purposes’ at an annual meeting of the Sunday Fund. The Metropolitan Radical Federation also petitioned the Prince of Wales in 1900, objecting to the contributions voluntary hospitals made to medical schools, and implying that hospitals engaged in human experimentation.42 Sir Henry Burdett had little time for the antivivisectionists, but he agreed that it was wrong for a hospital committee to devote any portion of the funds subscribed for the relief of the sick to the purposes of medical education. He regretted that some hospitals had ‘very weakly’ given grants to their schools. The hospitals had suffered financially from Coleridge’s attacks, and had it not been for the education issue the antivivisectionists would have had no case against the hospitals.43 In the light of the pledge that the Prince of Wales had given37, the King’s Fund established a committee in 1904 chaired by Sir Edward Fry and including the Bishop of Stepney and Lord Welby, to determine whether any money subscribed for the relief of the sick poor to any of the twelve teaching hospitals had been contributed to the hospital medical schools. The Fund gave the teaching hospitals less than a month to produce their accounts, and to comment on the mutual benefits the hospitals and schools gained from their association. At Guy’s, the dean maintained that it was impossible to separate the provision made for the relief of the sick from the steps taken in the furtherance of medical education. Every dressing and every examination had as its chief purpose the treatment of injury or disease, but was also of educational value. When he came to give evidence Stephen Coleridge tried to raise the vivisection issue, saying that had he not discovered that medical schools undertook vivisection he would never have become interested in their finances or started the agitation against them. He again insisted that the medical schools were only receiving support from their hospitals because the King’s Fund had increased their income. The committee worked rapidly and within a few weeks reported that two hospitals were not subsidising their schools out of hospital funds, two others were not clearly deriving a benefit from their hospitals, but that the remaining eight were receiving direct or indirect cash benefits. The report drew attention to the ‘intimate and complex relations’ between the schools and the hospitals, which made it impossible to draw up a cash balance of the more intangible benefits given and received by each. The committee felt that the mutual benefits balanced, and the hospitals should not, in addition, make cash contributions to the medical schools, save for specific services the schools performed to assist the treatment of patients.44 Mr Perry, writing from the Counting House at Guy’s to Danvers Power of the King’s Fund, said that whatever action the Fund proposed to take on the report should be taken promptly, at the next distribution. Otherwise Stephen Coleridge would have a reasonable grievance and would be on the warpath again, drawn sword in hand.45 The Fund did not ignore the great importance of medical education, believing that the facilities afforded by the voluntary hospitals placed the whole community under a heavy obligation, but it became the Fund’s policy to ensure that its grants were used solely for the purpose of patient care. Each year the hospitals had to submit a statement that no payment had been made to or on account of the medical school out of the general funds for the relief of the sick poor. Hospitals and schools were asked to keep separate accounts. During a dispute that rumbled on for a number of years the King’s Fund withdrew its annual grant to St George’s because the hospital appeared to be paying the medical school laboratories far more for their services than other hospitals.46 Some hospitals wished to continue to assist their schools, not least because the schools annually supplied them with junior staff. The hospital authorities sometimes approached subscribers asking them to agree that in future their contributions could be paid into a ‘discretionary account’. They could then be passed to the school if the house committee wished.22 The King’s Fund was always careful to maintain the distinction between the finances of the hospitals and those of the medical schools. Many years later it was still found necessary to produce a printed policy statement to issue to hospitals. In 1929 when St Bartholomew’s launched a joint appeal for hospital and medical school it came into conflict with the King’s Fund.47 Yet medical school staff were not lacking in supporters. When the Research Defence Society was formed by the medical profession, Sydney Holland of The London Hospital became its chairman. He made it his business to satisfy himself that the research workers at his own hospital were not ‘cruel monsters Thereafter he defended medical research in private, in public and later in the House of Lords. Year after year he fought a bitter controversy with Stephen Coleridge in the press, although in private they were good friends respecting each other’s point of view. And when Stephen Coleridge himself lay ill, Sydney Holland made a point of visiting him. The medical course became considerably stiffer during the second half of the nineteenth century. The facilities for scientific and clinical instruction were improved, at considerable cost. The private medical schools disappeared, and the medical schools of the great hospitals reigned supreme. The number of students entering the hospitals each year could be calculated from the information supplied to the Royal College of Surgeons, which collected the numbers for the Government Inspector of Anatomy Schools. The figures showed that the intakes rose progressively between 1850 and 1880, but thereafter the numbers fell.
By the early 1900s the London intake had fallen below 300 a year. While all the country’s medical schools were affected, those in London were particularly hard hit. The financial viability of some of them was threatened. The dean of Charing Cross Medical School attributed this fall in numbers to the developing competition of provincial medical schools, the abolition of pupilage as a method of entrance to the profession, the effect of lengthening the course in 1894 from four to five years which had greatly increased the cost of a medical education and bad publicity resulting from the continuous campaigns in the latter years of the nineteenth century to reform medical education in London.48 A long standing problem faced by London medical students was the difficulty of the examination for the degree awarded by the University of London. The standard was recognised to be higher than that of the provincial and Scottish universities. Most medical schools therefore prepared their students for the more practical diplomas of College and Hall, or Conjoint. Only a small minority of students proceeded to take the university degree and schemes for university reform generally aimed to make it easier for students to obtain degrees, as well as to enable the university to teach in addition to examining. Some reformers, believing that it would never be possible to change the way in which the University of London operated, proposed the establishment of a second university in London or the granting of the right to award degrees to the Royal Colleges.49, 50 The evidence given to the Select Committee of the Lords (1892) revealed the differences between those wanting a central academic establishment and those seeing medical education in more practical terms. Some favoured a degree of amalgamation of the smaller schools, particularly of their preclinical departments, and the Lords had recommended that if schools affiliated like the colleges of a university they might form a teaching institution able to afford and secure good lecturers. Much of the pressure for a ‘teaching university’ came from the need felt by the teachers to have some control over the content of examinations. Medical schools sometimes maintained that they were forced to follow a syllabus drawn up by university staff who might be less experienced than the schools’ own teachers. The constitution of the University of London was altered by Act of Parliament in 1900. The university rapidly established a faculty of medicine and appointed teachers, but the formal links established did little to alter the independence of the hospitals’ schools. The curriculum was becoming crowded because of the pressure to include new subjects, and the expense of pre-clinical instruction was continuing to rise; indeed the cost of the pre-clinical course had trebled because of the need for laboratory facilities. As the schools had no financial reserves the teachers of pre-clinical subjects had to rely on the generosity of their clinical colleagues, or work largely at their own expense in the hope of future advancement. There was increasing recognition of the desirability of separating the pre-clinical subjects for which laboratories and specialised staff were required from the clinical years when students were mainly taught in hospital.51 In 1902 the faculty of medicine drew up a ‘concentration’ scheme for an Institute of Medical Sciences, to be located in South Kensington, which would teach physics, chemistry, biology, anatomy and physiology to all students, whichever hospital they proposed to enter and whatever examination they wished to take. An appeal was launched the following year and £70,000 was collected. However the concentration proposals met with opposition, notably from St Mary’s, St. Bartholomew’s and The London. King’s College and University College also saw it as a threat to their well established science faculties. In 1907 the faculty of medicine changed its mind, and the money collected had to be returned to the donors. Meanwhile, Sir Donald Currie gave £80,000 to University College Hospital to provide a new medical school and, at the suggestion of the university, agreement was reached in 1905 that Westminster Hospital students would receive their pre-clinical education at King’s College, and those of St George’s either at King’s or University College. Charing Cross made a similar arrangement in 1911, the students beginning their studies at King’s College, ‘enjoying the advantage of becoming University students in the true meaning of the term’.48 Vacated space in a hospital seldom remains empty. As the students moved out of the laboratories the Charing Cross pathologists moved in. The new constitution of the University of London was in the nature of an experiment, intended to reconcile conflicting interests by creating a body on which all were represented and which had supreme authority. It proved unable to conciliate the interests or exert authority - certainly not in medicine. Only three medical representatives sat on the senate, so nine schools had only the most indirect contact with policy making. In 1908 the possibility of a royal commission began to be discussed.52, 53 A commission was established the following year under the chairmanship of R B Haldane, the Liberal politician and a life-long friend of the Webbs. The remit of the commission covered all faculties, but medicine received particular attention. Three of the most important witnesses were the physiologist Professor Starling, Abraham Flexner and Sir William Osler. Sir William Osler was a strong supporter of the university ideal of combining teaching with the advancement of learning. He had been concerned with the development of the Johns Hopkins Medical School and had precise ideas about the organisation of teaching, research and professorial clinical units. ‘The hospital’, he wrote, ‘should become part of the university system. It is a great laboratory in which we collect for rectification the experiments which nature makes upon us. The study of disease is just as much part of university work as is the study of mathematics, and a close affiliation of the two institutions (school and hospital) is the best guarantee of that combination of science and practice which is the right of people at the present day to demand.54, 55 Abraham Flexner, whose account of European medical education had been influential in the reform of medical education in the USA, drew attention to the unevenness of laboratory development, good at University College, reasonable at King’s, Guy’s and The London, but otherwise inadequate. Flexner said that in the clinical departments the typical English physician was still of the intelligent empirical type; once on the staff he gave up the laboratory and with it the laboratory state of mind. Teaching offered incidentally by hospital staff could not be of university quality. The relationships of London students to their hospitals deserved to be copied, but the merits of the system were used as excuses for not attempting anything better.56 The closely reasoned report of the royal commission appeared in 1913 and the unanimous conclusion was that the organisation of the university was fundamentally defective and that it could not develop into the type of university the capital city of the Empire should have. The report stated that the university had signally failed to gain the sympathy of the medical schools. The commissioners wished to see preliminary scientific studies undertaken at school and they did not want the preclinical sciences concentrated into a few institutions; Flexner had criticised the separation of pre-clinical laboratory sciences from the wards of a hospital. Radical changes were suggested for the clinical years. While paying tribute to the practical experience of London students, the royal commissioners said that such ‘professional’ training could never substitute for university education and the stimulus of working with teachers selected for their academic achievements, actively engaged in research. A consultant in busy private practice could not devote enough time to the development of his subject or serve adequately as a university professor. The main theme of the report was, therefore, the excellence of the London clinical tradition but the extraordinary inadequacy of support for laboratory work and the research required for the promotion of medical education.57 The remedy proposed was to institute chairs in clinical subjects, form university medical colleges and introduce academic staff into the hospitals. A professor with a staff of assistants would control wards and an outpatient department, and would have laboratory accommodation for investigation and research. Students would be attached to the academic unit in the same way as they worked for consultants in active practice. It was suggested that perhaps three of the medical schools, with their attached hospitals, should be incorporated completely into the university. These far reaching proposals aroused great controversy. How would the university obtain financial and educational control of one or more of the medical schools which were in fact part and parcel of the hospitals? It would mean controlling the hospitals themselves while the hospital administration would have to continue to raise the money to keep the hospital going. The decision of the King’s Fund following the report of the Fry committee to withhold grants from hospitals which made contributions to their schools from the general funds was an added complication. To run a medical school was no longer a profitable occupation. In many schools the staff had looked to the hospital for assistance in maintaining its viability. This had been the reason for the scheme to concentrate the preclinical sciences. House governors could see the economies which would result if every hospital did not have to support an expensive preclinical department.51 The process of selecting three schools out of twelve for full incorporation into the University was likely to be controversial. It would largely limit the selection of academic staff to those already working in the chosen hospitals, and there was more than a suspicion that the University would look no further than King’s College and University College Hospitals. To divide the teaching hospitals into sheep and goats in this way was to few people’s liking. It would also prove difficult to persuade governors, whose primary objective was the treatment of the sick poor, to continue to finance a hospital under university domination. Finally, if academic units were to be established they would require as many as two hundred beds to cover medicine, surgery and gynaecology. Only a very large hospital could provide this number if any room was to be left for the existing honorary staff. The staff in many of the teaching hospitals did not accept that the picture was as black as Haldane had painted it, and teachers recoiled from the thought of entirely science-based and laboratory-educated doctors. The medical faculty of the university disagreed with the proposal that professorial units should be concentrated into three constituent colleges and thought they should be distributed amongst all the medical schools. The faculty concluded that it was undesirable to limit the scope of university influence by confining university medical education to three colleges. 8 However the Board of Education accepted the main thrust of the Haldane Commission and established a committee to consult on practicalities. One new source of money appeared. In 1908 St Mary’s Medical School successfully applied to the Board of Education for a grant under the Regulations for Technical Schools. In 1909-1910 eight schools in London received grants. Sir Robert Morant at the Board of Education considered that medical schools were just as entitled to financial aid as courses in engineering, architecture and mining. The state now regulated the qualification of the profession through the General Medical Council, and directly or indirectly was increasingly becoming an employer of doctors. It had need of adequately trained medical men. Postgraduate study By the 1890s there was increasing recognition that the development of postgraduate study would benefit both doctors and their patients.60 At first postgraduate education was mainly tailored to those with specific needs, for example those proposing to take up a post in the colonies. Jonathan Hutchinson started a series of afternoon demonstrations at his personal clinical museum in Great Portland Street and soon after, in 1899, obtained a building in Chenies Street. In association with some of the medical schools he organised the Medical Graduates College and Polyclinic. The West London Hospital was also early in the postgraduate field, beginning courses in 1893. These proved so popular that the hospital provided library and lecture theatre facilities in a new building specially erected in 1901. At much the same time the London Postgraduate Association was founded ‘to make the wealth of London’s clinical material available to practitioners’. The Association made arrangements with Charing Cross, Guy’s, King’s College Hospital, St Mary’s, St Thomas’s, the Westminster and University College Hospital, as well as with some of the special hospitals like the Brompton, Great Ormond Street, the National Hospital for the Paralysed and the London School of Tropical Medicine. For ten guineas a ticket would provide admission to all of them for three months. Other courses became available at the North East London Postgraduate College at the Prince of Wales’ Hospital in 1902, and the London School of Clinical Medicine (the Seamen’s Hospital) in 1906. The value, and in some circumstances even the necessity, of postgraduate education, was so widely recognised that there was no need to dilate upon it, said the British Medical Journal in 1908.61 The rapid progress of medicine called for a system which would enable all experienced practitioners to keep up to date. There was more to know, a more widespread desire to know, and a greater readiness on the part of those who knew to teach. Most of the courses did little more than provide local practitioners with an educational stimulus. The contribution made by the University of London to postgraduate study was even less than to the undergraduate course and organised postgraduate education was hardly a success story considering facilities which were available. An article by Hawthorne suggested that there should be at least be a central bureau to provide information on the courses available, and cooperation in time-tabling.62 The erection of a new hospital as a postgraduate clinical centre might not be a practical possibility, but some general hospitals had very few undergraduate students. Might not one see that it would do better as the clinical centre of postgraduate education? It would need to be in the middle of town so that it could work with the special hospitals which were valuable sources of clinical experience, often with schools of their own. Such a development would make London the centre of postgraduate education in the English-speaking world, but in The Lancet’s view there were problems in Hawthorne’s plan. A hospital which welcomed all the best teachers in London would place the existing medical staff in an invidious position, and ill-feeling would be inevitable. Nevertheless, said The Lancet, all practitioners had a right to expect facilities which would help them keep abreast of the strides being made in scientific medicine.63 The clustering of hospitals in the middle of London had been the subject of adverse comment for fifty years. The point had been made by Florence Nightingale, for the third edition of Notes on Hospitals contains maps showing the concentration in the centre of London and Paris. A fall in the population of central districts occurred in every decade from 1871, partly as a result of slum clearance schemes and the development of railway and tram systems, exacerbating the problem. The 1891 census showed a dramatic change in demography of London and other major cities, see Figure below.64 Growth in London was concentrated in an ‘outer ring’, in places like Leyton, Willesden, Tottenham and West Ham. The population of the Cities of London and Westminster, the Strand, and St Giles, showed a marked decline. Ten years later a further census confirmed the trend and the realities of metropolitan development became widely recognised. No more than a third of the growth which had occurred within fifteen miles of Charing Cross had taken place within ‘London proper’.
In April 1902
Mr Peyton Beale, a surgeon at King’s College Hospital, wrote to The
Lancet that
before the twentieth century was far advanced the problems of
hospital accommodation in London would have to be faced. The
residential areas had changed and cheap and rapid transport
facilities had been developed. The sick poor should be able to
obtain relief near where they were living; those seeking medical
education should go to the places where the sick poor were, and
not expect the sick to come to them from afar off. The
alternatives were to transfer great general hospitals away from
the centre of London, or to build new general hospitals further
from the centre.65 Population trends in the metropolitan boroughs, 1899. It was said that hospitals needed rebuilding every hundred years, as developments in medical science outstripped the facilities available. The clinical activities of the hospitals were changed out of all recognition by anaesthesia, antisepsis, specialisation, the growth of outpatient departments and subsequently radiology. St Thomas’s had been rebuilt and, as a result of the generosity of Sir Blundell Maple, University College Hospital was being reconstructed. But Charing Cross, the Westminster, King’s College Hospital, Gus’s, St George’s, St Bartholomew’s and The London all faced problems. The question of relocation was frequently raised but governors of a hospital had no obligation to areas other than their own. There was a fear that a new district might not give adequate financial support. A hospital might also lose its traditional supporters. In spite of pressure from the King’s Fund, Charing Cross Hospital held to a decision taken in 1896 to expand into new buildings in King William Street. The Fund’s visitors reported in 1898 that nothing could make the present building suitable for hospital purposes, and that in their view it should be pulled down and rebuilt elsewhere. 66 the hospital did not agree. Alfred Saxon-Snell, son of Henry Saxon-Snell, was appointed architect and fund-raising began.
Members of the theatrical profession, with which the hospital was closely associated, gave their services and a grand bazaar was held at the Albert Hall. The report of the King’s Fund for 1902 included a request that any proposal for a new hospital, or for reconstruction or a major extension of an existing one, should be submitted to the Fund before definite action was taken, in the hope of improving the distribution of beds. The Fund’s distribution committee adopted a policy of supporting amalgamations, setting aside £5,000 to assist in the process. During 1903 discussions were held with orthopaedic, ophthalmic and ear, nose and throat hospitals. The report for 1904 suggested that those hospitals which devoted themselves entirely to one disease should work ‘under as few roofs as possible’. It was implied that a judicious reduction in the total number of small hospitals might be advantageous. The prince referred to the high sense of duty of those hospitals which, by amalgamating, subordinated their private interests to those of the whole system. The argument for relocation was taken up in 1902 by the newly formed Hospital Officers Association*, a group within which ‘progressive ideas and practical information about hospitals’ could be disseminated to arouse keener interest in the medical charities. Its inaugural lecture was given by Mr Adrian Hope, secretary of the Hospital for Sick Children, and was concerned with the future of the voluntary hospitals. Hope believed that the King’s Fund would become increasingly influential. He also thought that some hospitals would have to consider selling their present sites and using the money to rebuild better premises on less expensive land. Many London hospitals were in need of rebuilding to modern standards, reflecting the demand from doctors for better conditions. Decisions should take account of rehousing; for instance, the London County Council was moving 40,000 out to Tottenham.67
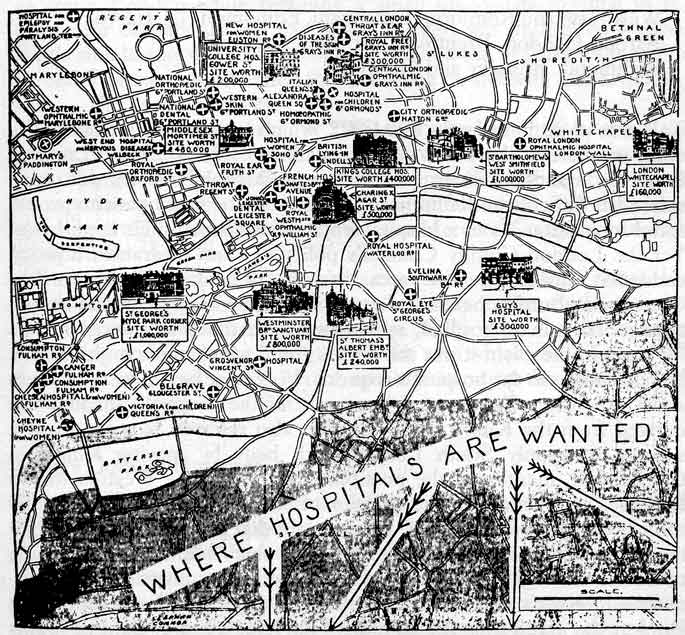
The medical
press paid little attention to Hope’s lecture, but the proposal
to relocate hospitals was picked up by the Daily
Mail which published a map showing the value of
the existing sites of the hospitals, and where they might be
moved to on Thursday 27th November 1902. . ‘Control and
organisation is necessary in any case’, commented the Mail. An
active correspondence followed.68 Correspondents
were virtually unanimous that relocation was a financially
viable proposition. The Westminster Hospital stood in Broad
Sanctuary, opposite Westminster Abbey, on a site worth £750,000.
If the sale could raise only half a million, the two hundred and
twelve beds could be rebuilt for £168,000 at Tottenham on a site
four times as large, leaving adequate money to endow beds and
meet running costs. Charing Cross could be rebuilt to serve the
new population around Woolwich for £145,000, providing 175 beds.
St Bartholomew’s, because it was ‘a large hospital and could not
be moved so far’, might go to Clapham - ‘a good central
position’.69 The relocation would cost
£550,000 but the sale should raise £1 million. Costs of
rebuilding were estimated to be £700 per bed. The secretaries of hospitals which had been relocated supported the proposal but the great hospitals, whose removal was being proposed, were rather less than enthusiastic. Sir Edmund Hay Currie of The London Hospital and the Sunday Fund told the Hospitals Association that the transplantation of ancient charities must be approached in the most gentle manner possible.70 Sir Trevor Lawrence, treasurer of St Bartholomew’s, wrote to the Daily Mail to point out that the dense local population, the ever increasing workload, and the need for West End physicians and surgeons to be near at hand — impossible if the hospital moved to Battersea, Greenwich or Tottenham — made its present position absolutely necessary. ‘No greater injury could be infficted upon the sick and suffering poor of the City of London than to move it from the site where it has done incalculable good.’ In reply the newspaper analysed the population of the City, Finsbury and Holborn and showed that it totalled 200,000; ‘on the accepted basis of one bed per thousand inhabitants’ the district was over bedded. Guy’s, King’s, Charing Cross and the Royal Free with a further 1,200 beds lay within one and a half miles of Bart’s. They were able to serve a population of two million where barely half a million lived. The paper also ran a news item about an aged plate-layer who broke his legs on Bexley station and had to be transported to Guy’s, fourteen miles by rail. The secretary of the Metropolitan Hospital, which had already been relocated, wrote to say that his staff had no difficulty in reaching the hospital as they were on the telephone. The matron at Tottenham said that their surgeon could ride his cycle rapidly through the quiet streets at night. The correspondence had served to emphasise what those working in hospitals had known for twenty years: that the population which had been moved as a result of slum clearance or the construction of new buildings was often poorly served; the economics of removal might often be sound; and that hospitals which had been moved were generally content. There was no doubt that they had gained in usefulness and in most cases the costs of rebuilding had been paid off. The Times carried two articles on 7 and 8 January 1903, commenting on the cramped site of St Bartholomew’s and the need for better accommodation if the future of the hospital and its school was to be assured. An editorial in The Hospital referred to the press coverage and stated that some pains had been taken to ascertain the facts. However much was spent on reconstruction at St Bartholomew’s the hospital could never be brought up to the standard of a newly planned building. In any case the census showed that the population of the City was falling. It would seem better to sell the site and rebuild in Old Street on the site of the old St Luke’s Hospital, next to the City of London Lying-in Hospital.71 In March 1903 Sir Henry Burdett addressed the Hospitals Association on the removal of large hospitals to congested districts or to the country. Sir Henry gave bed ratios for five concentric districts:
Taken as a whole the ratio was 1:922, which is remarkably close to the usual estimate of the needs of a population — 1:1,000. South London, Battersea and Tottenham had the greatest problems. Burdett considered it difficult to define hospital districts, for many patients would travel long distances to a hospital which commanded their confidence. Yet the London County Council’s policy of slum clearance, housing residents outside its own area, created difficulties in places like Tottenham. Burdett believed that the London County Council should finance Tottenham hospital, as its planning had created new demands for care. In the event it was the King’s Fund which came to the rescue by responding to the hospital’s requests. Very large grants were made to assist expansion. Soon over 50 per cent of the hospital’s income was derived from the King’s Fund. Burdett also referred to a report of a scheme to supply South London with beds by moving King’s to Camberwell, mentioned the possibility of moving the Westminster to Battersea, and hedged on the question of St Bartholomew’s. In the lively discussion which followed one speaker said that though City sites might be costly, there could be no better use for valuable land than the saving of human life. Sydney Holland of The London supported the amalgamation of King’s and the Westminster on a suburban site, but when Burdett was asked what the attitude of the King’s Fund might be to this proposal, the question was ruled out of order.70, 72 Amalgamation, rebuilding and removal Each of the great hospitals was in a different situation and each had to decide how best to resolve its problems. St George’s and King’s were on cramped and crowded sites and reconstruction where they were was virtually impossible.70 St Bartholomew’s and The London had more ground and wanted to rebuild on site. Both found it necessary to launch appeals to finance modernisation and were in direct and bitter competition with each other. St Bartholomew’s mainly needed a new casualty department and accommodation for the special departments. This was made possible by the acquisition of part of the adjacent site of Christ’s Hospital, the remainder being acquired by the Post Office. The decision provoked such public criticism that a committee was established by the Lord Mayor to review the question. Witnesses pointed to the large working population served by the hospital, but Sir Edmund Hay Currie thought money would be better spent on a new site in north or south London while retaining a small up-to-date hospital in the centre for outpatients and casualties. Burdett was undecided — either Bart’s should stay where it was or be rebuilt on the St Luke’s site in Old Street. The committee settled for rebuilding on site with one dissenting voice — Sir Savile Crossley.” St Bartholomew’s appeal for £400,000 was launched by the Lord Mayor, with the sanction of the Prince of Wales and the support of the press. Sir Trevor Lawrence spoke of the great difficulties which would be experienced by the sick poor if the hospital moved, and the appeal was supported by the Chief Rabbi and the Mercers’ Company, amongst many others.73 St George’s Hospital established a committee to consider removal to a suitable site within the area it served, mainly to the south-west, but problems arising from dual ownership of the site, the difficulty of rebuilding and endowing a hospital on the sum which could be realised from the sale, and a division of opinion amongst the medical staff brought the scheme to a halt.74 King’s College Hospital The chairman of the committee of management at King’s College Hospital, Lord Dillon, opposed removal. However, many of the medical staff recognised that there was over-provision in central London and that the construction of Kingsway from the Strand to Holborn had led to the removal of many of the poorer inhabitants. The existing buildings were ‘obsolete in design and inadequate in accommodation’, the existing site was small and upgrading to modern standards was impossible. Finally, Charing Cross Hospital had recently been enlarged and the City of Westminster was over-rich in hospitals. In May 1903 the hospital council asked a special committee, including representatives of the King’s Fund and the Mayors of Camberwell and Southwark, to consider the practicalities of moving King’s.75 The report, presented in July, was favourable. A site near Camberwell was given to the hospital by the Hon W H D Smith MP. It was in an area which had been identified by the select committee of the Lords as in need of a large general hospital. The governors, knowing the views of the King’s Fund and that the King himself was in favour, petitioned the King and the Prince of Wales in November 1903, seeking agreement to removal and help in raising the £300,000 it would cost. The Prince of Wales approved entirely and the King’s Fund made a large grant. At a meeting at the Mansion House the following March, the Archbishop of Canterbury proposed a motion approving removal, and financial support was pledged. The King’s Fund made significant contributions to the removal fund each year. A notable fund-raising event was an Elizabethan Fair — ‘one of the most brilliant social occasions of 1906’ — held in the grounds of Lincoln’s Inn Fields. The Duchess of Connaught, the Lord Mayor of London and the ambassador of the United States opened one each of the three days it lasted. The King’s—Westminster scheme Shortly after the decision was taken to move King’s College Hospital the relocation of the Westminster became an issue. The hospital, in Broad Sanctuary, had undergone major reconstruction in 1877 but the building was far from satisfactory. The first report of the visitors of the Prince of Wales’ Fund drew attention to the need for greater space but expansion was impossible; the hospital was in a strait-jacket.76 Some of the staff saw that a hospital of modem standard could only be achieved by relocation and Sir Henry Burdett thought it might be a good idea, despite the financial problems, if the Westminster could move to Battersea and amalgamate with the Bolingbroke.” A merger between the Westminster and King’s College Hospital was suggested by Sydney Holland of The London, writing to Sir Savile Crossley at the King’s Fund. Several of the London hospitals were appealing for funds and this amalgamation would reduce the number of appeals. Holiand thought it was a real scandal to have so many hospitals crowded together, while other places had none at all. If the Westminster could be persuaded to throw in its lot with King’s the joint investments of the two hospitals would guarantee the success of the scheme. Believing that his association with the proposal would doom it to failure — a merger would make the position of The London easier — Holland suggested that the idea should come from elsewhere. He thought that Burdett would oppose any proposal he made and a scheme of this magnitude could not be carried through by ‘ordinary humdrum, respectable methods’. The Prince of Wales agreed to raise the matter at a council meeting of the Fund, but it provoked opposition and a communication from the palace in June 1904 recorded that the King was sorry to hear that the Westminster had decided to oppose amalgamation. However his majesty hoped that the number of medical schools might be reduced.78 ‘The path of the amalgamator is thorny’, commented one member of the council of the King’s Fund. Westminster — St George’s The reunification of the Westminster and St George’s — separated for 180 years — looked a better proposition, at least initially, when discussed in 1913. A committee was formed to consider the development of a joint hospital of at least 300 beds, either at Clapham or Wandsworth Bridge, using funds released by the sale of both sites. There was every chance of success. It was generally recognised that many of the patients attending both hospitals came from Clapham and Wandsworth. The poor had largely disappeared from the neighbourhood of St George’s and the area round the Westminster was served by other hospitals like Charing Cross. The proposal was widely welcomed and Sir Henry Burdett supported it in The Hospital. The Lancet commented that hospitals could not now live by ministering to highly paid domestic servants whose needs were catered for by the National Insurance Act. The King, patron of both hospitals, commanded that a letter be written stating that their majesties were most gratified to learn of the proposed amalgamation, which was likely to be for the greater benefit of the sick and suffering poor. Early enthusiasm for the project faded once a dispute arose on the choice of a site.79 The St George’s representatives and the medical staff of the Westminster voted for Wandsworth where a piece of ground was available between the gas works and the distillery. This was opposed by representatives from the Westminster on the grounds that a site at Clapham was nearer the existing positions of both hospitals and also to Harley Street. An analysis of patients’ home addresses showed that more lived near Clapham than Wandsworth. The Westminster house committee refused to ratify the majority decision, and the King’s Fund offered its ‘good offices’ in an attempt to settle the difficulty. The King himself studied the papers with interest, and much preferred the Clapham site. Relationships between the hospitals became strained. The chairman of the Westminster, believing that his hospital could not wait for St George’s, bought the ground at Clapham to keep the option open while discussions proceeded. By May 1914 the Westminster was designing a 300 bed hospital for the Clapham site with the agreement of the King’s Fund. The outbreak of war put an end to immediate prospects of a building appeal and the opportunity to sell the site in Broad Sanctuary.76 A successful amalgamation Sometimes the King’s Fund succeeded in achieving an amalgamation, as in the case of the small orthopaedic hospitals. There were three, the City, the National and the Royal. In 1903 both the City and the Royal wished to rebuild, but the Prince of Wales, strongly in favour of amalgamation, was unwilling to lay the foundation stone of either if they rebuilt separately.80 A meeting of the Royal and the National with the City agreed in principle that there should be a joint development with a town branch and a convalescent branch in the country. Because of its financial resources the King’s Fund was able to make grants contingent upon a merger and to see the hospitals through if their combined funds were insufficient. Agreement was almost in sight when the City hospital reneged on the deal. Not only was the King’s Fund irritated but the recalcitrant hospital found that it had lost its grant from Hospital Sunday as well. The palace thought that the refusal to cooperate was ‘monstrous’ and the Princess of Wales intimated that she was unable to attend a charity performance in aid of the City hospital. The King’s Fund decided to support the more limited merger. ‘It will cost a great deal of money’ said a council member, ‘let us hope it will be money well spent.’81 The door was left open for the City to join on equal terms at a later stage and this happened. The amalgamated hospitals received a new charter in 1905 as the Royal National Orthopaedic Hospital. The new building in Great Portland Street was opened in 1909 by King Edward VII and Queen Alexandra. The Fund worked hard from 1903—1914 to secure the unification of the five ear, nose and throat hospitals, but this proved impossible.82 However it expressed great satisfaction at the unification of the London Throat Hospital with the Hospital for Diseases of the Throat, Golden Square, two hospitals which were the result of an earlier feud. It supported the unification of University College Hospital with the National Dental Hospital in 1914, and with the Royal Ear Hospital in 1918. The nature of the voluntary hospitals made amalgamations a slow process. The King’s Fund was advised by its executive committee not to take the initiative with amalgamations. It was widely believed that a hospital’s income was intimately related to its site. Hospitals that moved some distance seldom seemed to take their subscription lists with them. When King’s College Hospital went to Denmark Hill it had great difficulty making ends meet, but Charing Cross which rebuilt in the Strand succeeded in paying off its debts, albeit after several anxious years. The financial affairs of the hospitals In spite of the hard work of the central hospital funds the financial position remained parlous. Revenues rose but the hospitals developed an increased appetite to spend’. Burdett demonstrated that the case load of the inpatient and outpatient departments was increasing faster than London’s population and that the cost of treating each case was also rising, a poor return he thought for all the effort put into fund raising.84 ‘ Sometimes the hospitals received massive individual bequests. In 1900 Professor David Hughes left something approaching £400,000 to the Middlesex, The London, King’s College Hospital and Charing Cross. The Lancet praised both the intelligence of his choice and his wish that a third of the income from the bequest should be added to the hospitals’ capital accounts. In the same year Mr Rudolph Zunz of Wimbledon left £100,000 for the endowment of wards in the name of his late wife Annie. Thirty four hospitals ultimately benefited and many have an Annie Zunz ward to this day.85 Few hospitals were adding to their capital and most were increasingly in debt. Their managers seemed to make a trade of poverty and those who succeeded in spending less than they received took great pains to conceal the fact from their subscribers.86 The leading and most successful exponent of the method of spending to the hilt and then appealing for support was The London Hospital, which, thanks to the energy and quality of its officials and chairman, was able to carry on this dangerous game with comparative success. Sydney Holland, speaking of the continuous efforts which had to be made to raise money, said that 55,000 personal letters produced only 2,500 answers. In his experience it took one mile of writing to raise £200. The secretary of The London believed that if a hospital was seen to be an asset to society, the money would be raised. For voluntary hospitals the rule was ‘that income would follow usefulness and efficiency.' 22 With the unceasing anti-vivisection campaign hindering subscriptions, the cry for help became increasingly acute, ‘implying a burden which threatened to become intolerable and imperil the voluntary system of support which had hitherto been little less than a national glory’.87 Speaking at the annual meeting of the King’s Fund in 1906 the Duke of Fife said: ‘There is one thing which nothing seems to overcome, and that is the apathy of Londoners with regard to their hospitals. The great majority of them do not subscribe and the plain truth is that the London hospitals are maintained by a small number of charitable people.’ The business of hospital maintenance ‘There is a type of philanthropist’, said Burdett, ‘who deserves to rank as high as the cheerful giver — the careful giver.’88 The task of the careful giver was made easier by the tables in Burdett’s Hospitals and Charities which was now joined by a new publication, the annual statistical reports based upon the returns to the King’s Fund. The first report, which analysed expenditure but not income, appeared in 1903 and contained details from 16 hospitals.89 It was confidential and was circulated only to those hospitals who had contributed. Each hospital agreed that it would not publish the figures, which provided a useful tool for internal investigations. UCH discovered that its expenditure was above average and it was paying excessively for beef; an investigation was set in hand and the contract price was obtained from The London for comparison. The reports, issued to the public from 1908, were based upon a revision of the uniform accounting system which was used by all three central funds.90 Comparison of cost per case and cost per bed became progressively easier but a series of articles on financial aspects of hospital management published in the British Medical Journal drew attention to the problems of comparing hospitals which differed in size, the seriousness of the cases admitted and the quality of the equipment and supporting services which they possessed. The Hospital considered that two tentative conclusions emerged from the analyses.88 One was that a hospital tended to be more expensive to maintain when a medical school was attached to it; the other was that outlying hospitals seemed cheaper per occupied bed than those nearer the centre of London. It had often been argued that the work students carried out as dressers saved on nursing costs, but the figures suggested that nursing costs might actually be higher in hospitals with medical schools. Neither was it clear that the free care provided by the honorary medical staff resulted in financial gain. A large and eminent staff ‘often meant expense in many directions’. The lower cost of suburban hospitals was easier to explain; all kinds of work were carried out more cheaply away from the centre. Useful though such comparisons might be, account had also to be taken of the effect on hospital costs of the advances in medical treatment.91 Listerian techniques had vastly increased the costs of operating theatres, although resulting in a widening of the scope of surgery and faster recovery for the patients. The London Hospital had doubled its throughput, halving the length of stay. Hospitals had evolved into a kind of business involving three partners, each possessing rights. These were the patients, for whose benefit the hospitals existed, the medical staff providing the skill by which the patients were treated, and, finally, those who voluntarily provided the funds to be used by the other partners. Contributions were welcomed from all sources but the charitable were not always broadminded or altruistic. Contributors to Hospital Sunday took offence when hospitals, including The London, organised film shows on the Sabbath, to raise money and provide working men with an alternative to the pub.92 Working men, subscribing to Hospital Saturday, expected a quid pro quo as of right, and to have a say in management. They did not see their contributions as an act of charity but as a form of insurance. The British Medical Association continued its attempts to protect the livelihood of general practitioners by restricting the size of outpatient departments and income groups to whom they were available. The association held a conference of the medical profession and members of hospital management committees in March 1905. The following year it petitioned the Privy Council to withhold a charter of incorporation from the Hospital Sunday Fund on the ground that it did not use its influence to end hospital abuse and restrict outpatient departments to cases referred by general practitioners.93 The Charity Organisation Society also opposed a charter, believing that the Sunday Fund and the King’s Fund should amalgamate. At yet a further conference called by the British Medical Association in December 1906 Sir Henry Burdett proposed a motion approving proposals to limit the size of outpatient departments, seconded by the chairman of the Hospitals Committee of the BMA. The teaching hospitals could not accept this limit upon their freedom and the chairman of St Mary’s intervened. The meeting agreed that the proposals would receive further consideration, rather than a welcome.94 Sir Henry Burdett clashed with Sydney Holland, chairman of The London Hospital, at a meeting of the Hospitals Association a fortnight later. Sydney Holland said that he was not dependent on the praise or blame of Burdett or his paper The Hospital; nor was he dependent upon Sir Henry for his position in the hospital world - he was afraid it would not be a very high one if he was. Sir Henry had stated that because the population of London had increased 6 per cent in the last decade while hospital patients had increased by 23 per cent there must be hospital abuse. That assumed that all patients had been treated ten years ago who ought to have been treated. Sir Henry failed to see that times and hospital care were changing. The special departments had a particularly high rate of growth. The hospitals had not added new accommodation for their own amusement, but because the sick had to be provided for.95 The British Medical Association called one more conference in 1908 but the topic was becoming a little threadbare. Hospital representatives were conspicuous by their absence. Burdett said that the meeting was in the main a rebellion by general practitioners against hospital outpatient departments and did the hospitals little good.96 The King’s Fund decided to hold its own enquiry once the report of the Royal Commission on the Poor Laws had been published. It established a committee in December 1910 to consider and report ‘upon the circumstances and conditions tinder which patients were seen at the outpatient departments & London voluntary hospitals and the precautions taken to prevent the admission of persons who were unsuitable’. It was an attempt to resolve an issue souring relationships between general practitioners and the hospitals. The committee held 27 meetings and heard 48 witnesses. It was agreed that, ideally, outpatient departments should have a consultative role but witnesses could see no sharp distinction between suitable and unsuitable patients as far as their financial circumstances were concerned. The possibility of an external method of sifting the patients who were to be seen was considered, for example by relying on general practitioner reference. The argument for such a procedure was that once patients were allowed to come it was difficult to turn them away or to enquire into the means of the large number involved. However, the committee did not think it would be possible to close the free access of patients to hospital in the absence of a tried and trusted sifting mechanism. Instead preference was expressed for the approach of the Charity Organisation Society and the majority report of the Royal Commission on the Poor Laws - to rely on the almoner system to exclude those able to pay and the truly destitute, as well as those able to subscribe to provident dispensaries. The committee wished to see the development of provident dispensaries on a large scale because, with a national insurance scheme of some type, they would help to reform outpatient departments by providing an alternative form of care. In any case it was essential that the hospitals adopted a uniform standard of acceptance in the outpatient departments. But times and attitudes were changing. Increasingly people felt that the gospel of honest independence ignored the very reasonable view that society might choose to support those who, in bad times, could not support themselves — and without perpetuating the division between the destitute and the rest. The conception of the function of hospitals was widening; the introduction of new and costly medical treatments meant that only hospitals could treat some conditions, raising the income level at which a patient needing treatment had to be regarded as ‘necessitous’. The remedies proposed for ‘hospital abuse’ were ineffective. For thirty years the cry of ‘hospital abuse’ had been heard, said the Fabian Society, despite which there had been a steady rise in the numbers seeking relief. The solutions suggested were futile and displayed a great ignorance of human nature. Cooperation between general practitioners and hospitals was, in the Fabian view, only partially possible under the economic conditions of practice. A coordinated state service of medicine was the only solution they saw which would be in any way satisfactory.98 The Royal Commission on the Poor Laws (1909) This royal commission was appointed in 1905 at the very end of a parliamentary administration and reported four years later. There had been criticism of the poor laws from all sides, but precisely why the commission was established at this juncture is far from clear. Some saw a need to restate and reinforce traditional principles of destitution relief; others to challenge them. The remit of the commissioners was wide, and hospital affairs formed only a small part of their task. Although the two reports of the majority and minority had little immediate or direct effect on either the poor law infirmaries or the voluntary hospitals, they set the scene for future developments. The commissioners themselves were people of experience, distinguished as practical reformers and creative social thinkers. Several guardians were selected as commissioners, and they were inevitably committed to the principles of 1834. The guardians had become a powerful lobby with strong esprit de corps. Four senior officials from the Local Government Board were members; there were two economists, Charles Loch from the Charity Organisation Society, and leaders in social study and research like Charles Booth and Beatrice Webb. The commission was far less successful in its early impact than its predecessor of 1834.99 Then the principles gained widespread acceptance and were rapidly implemented across the country. In 1909 not only were the commissioners divided, but their divergences made the adoption of proposals based upon either the majority or the minority reports a serious and controversial matter. The campaign that the Webbs waged against the majority report, and in favour of the break-up of the poor law, further reduced the chances of legislation. The two reports had much in common. They condemned the existing system and wished to see an end to the mixed workhouses. Neither wished there to be indiscriminate relief without detailed investigation of the applicants. The majority report reflected the views of the Charity Organisation Society. It recommended the abolition of the guardians and the transfer of poor law responsibilities to new public assistance committees consisting of county and county borough council members with the co-option of representatives of local charitable organisations. Beatrice Webb’s minority report, instead of retaining the Poor Law in fact if not in name, wished the services to be divided amongst a number of expert and specialised agencies, so that the necessitous could be provided for alongside other members of the population. Underlying the minority report, and much of the Webbs’ thinking, was a belief that a certain measure of discipline, even compulsion, might be necessary for the public good. Citizens had to remember that they had duties as well as rights. Both reports, in the event, proposed radical solutions although the effectiveness of the Webbs’ campaign for the abolition of a destitution authority obscured to some extent the sweeping changes proposed by the majority. With so many problems to consider, it is hardly surprising that neither report said much about London’s hospitals. There was some criticism of the overlap of services. One of the commissioners, Norah Roberts, conducted a survey of the extent to which outpatients at St Mary’s, the Royal Free and St Thomas’s were also receiving assistance from the poor law. She found that 11 per cent were doing so and that there was ‘an extraordinary antagonism between the two agencies’. Relieving officers resented the work created by hospitals who applied for the removal from their wards of the homeless and encouraged patients to demand relief. The hospitals complained of the slowness of the guardians in coming to the rescue by accepting responsibility for destitute patients. Norah Roberts suggested that the relationships between the two organisations should be clearly defined by a disinterested and authoritative power.100 Both the boards of guardians and the voluntary hospital movement viewed the reports with suspicion. In April 1910 representatives of the voluntary hospitals met at Guy’s to re-form the old Hospitals Association, which Burdett, not unnaturally, considered responsible for much good work while it was an active organisation.101 Cosmo Bonsor, the president of Guy’s, became the president of the new association, and Burdett joined the council. Its objective was to provide a forum within which ‘organised institutional opinion’ might be developed, and its first action was to convene a conference in October 1910. The two key speakers were Charles Loch and Mrs Sidney Webb, representing the majority and minority factions. Each discussed the role they saw for the voluntary hospitals in the future, Loch considering that they might be institutions where people would be treated who could pay something towards the cost of their care, although not the full economic cost.10 Beatrice Webb started by postulating the existence of a ‘unified county medical service’ managed by local authorities. This service would include both the infirmaries, freed from poor law control, and those voluntary hospitals who wished to join. The voluntaries might treat particular types of cases within the scheme, perhaps those requiring the specialised attention available from their superb visiting staff. Mrs Webb said that any question of ‘nationalisation’ or ‘municipalisation’ was so remote from practical politics that it did not need to be discussed. If the voluntary hospitals treated patients free of charge, that would save the rates. If they wished to charge for their services, then the local health authorities might have the right to nominate a limited number of board members.103 A united county medical service was still a long way off, but the guardians could see problems ahead. With progressive improvements in staff and equipment the demand had risen, as it had for treatment in the voluntary hospitals. Increasingly the poor law infirmaries were serving artisans on good wages, as well as the truly destitute. Mr Lockwood, the Metropolitan District poor law inspector, recorded in his reports that there had been no reduction in the numbers seeking indoor relief, even though there had been no severe winter nor a depression in trade.104 He thought this was due to the excellent provision for the sick and the superior medical and nursing services now provided. Indeed he listed the many improvement schemes in progress: new infirmaries for Bethnal Green and Islington, extensions to Camberwell and Hackney infirmaries, and the purchase of a site for an extension in Whitechapel. The new infirmaries were well designed and the building cost was reasonable. The Local Government Board insisted upon a site large enough to allow a free circulation of air around the ward blocks. Architects were involved from earliest stages which did not happen when a voluntary hospital was to be built; a site might be bought on the advice of anyone but an architect and later found to be too small, as happened at King’s College Hospital, Denmark Hill.105 As a result of Miss Twining’s long campaigns nursing standards were also improving. By the early 1890s, according to her evidence to the Select Committee of the Lords11, it was rare for an untrained nurse to be appointed as matron of an infirmary in London. Pauper nurses were being withdrawn slowly and were barred in 1897, although they continued to act as assistants. The Central Poor Law Conference discussed the best way of supplying and training infirmary nurses at the Guildhall in 1899. Infirmaries were increasingly setting up their own training schools. At Lambeth the medical superintendent, the matron and the home sister gave lectures to the probationers in their off-duty hours. Before receiving their certificates they had to ass an examination usually conducted by a doctor from St Clinical services were expanding and although some patients would be transferred to a voluntary hospital if surgery was needed, serious operations were increasingly undertaken by infirmaries. In 1889, 128 operations were carried out at St Marylebone, of which 30 were major. In 1909 the figures were 386 and 79 respectively.107 Nevertheless the wards were crowded, particularly in the winter, and extra mattresses might have to be put down. The guardians varied in their strictness in testing eligibility of those applying for relief. In Islington they turned to the Charity Organisation Society for help in determining which applicants should be assisted from the rates, which qualified for charitable assistance, and which were well able to help themselves. The Lancet praised this action for ‘the rates of the parish were saved by it, and the poor were helped in a way agreeable to their self-respect’.108 While some of the larger provincial cities had also separated the sick from the general pauper population, the separate infirmaries of London had carried the process further than most other towns. Yet there were wide variations within London. Dr Thackray Parsons, the medical superintendent of Fulham, presented tables showing the staffing levels and the nature of the equipment of each infirmary, when he addressed Central Poor Law Conference in 19l0. He defended the more active boards of guardians like those of Hammersmith, who were criticised in the press for their expenditure. Construction costs of £350 per bed enabled the Hammersmith Infirmary to provide conditions of hospital standard for the treatment of patients ‘who were curable under good conditions’. Dr Parsons pointed to the differences in the type of case admitted to infirmaries. The average length of stay in the City of London Infirmary was 113 days, whereas at Fulham it was 40.4 days. There were twenty deaths each year for every 100 occupied beds at the City of London, compared with 129 at Fulham, which was clearly admitting patients who were acutely ill. Equipment at the infirmaries compared badly with the voluntary hospitals; most had operating theatres but many did not have a bacteriological laboratory or an X-ray department. The number of beds per nurse varied between 2 and 2.6 in the voluntary hospitals, while 8-10 beds per nurse was the rule in the infirmaries. Dr Parsons did not believe that the infirmaries should restrict themselves to chronic and incurable patients; there were so many acute cases in London that neighbouring voluntary hospitals frequently had to refer cases of burns, appendicitis, fractures and pneumonia to Fulham because their own wards were full. To solve the problem by doubling the size of the voluntaries was out of the question. Even were this to be done at the expense of the guardians, problems would arise, for state-aid would raise questions of governance. A better answer seemed to be to improve facilities, staffing and salaries in the infirmaries. Parsons foresaw the growth of a large public medical service in each county, providing a system of hospitals with specialist departments, sharing the work amongst themselves. If the separate management of each infirmary ceased and the hospitals of the Metropolitan Asylums Board and the infirmaries were brought under one centralised body, many advantages would follow. Joint specialist staff could be appointed, nurse training could be improved and better use made of beds. Situations sometimes arose in which one infirmary was crowded whilst its neighbour was half empty. Dr Parsons told the guardians that there would be advantages in concentrating all the poor law medical, public health and lunacy work under one committee of the London County Council. He would grant that the guardians had done good work but further improvements required a new administrative structure. During the debate which followed it was clear that the guardians did not agree that their staff were underpaid, for there was no shortage of applicants. Neither did they think that a change of administration was called for. Dr Parsons was thanked politely for his address. The National Insurance Act (1911) Before the Poor Law Commissioners had reported, old age pensions had been introduced and other measures followed. Lloyd George’s National Insurance Bill was an attempt to tackle the problem of ill-health which threw so many respectable people onto the poor law. The act provided insured workers with care from a ‘panel doctor’ but with the exception of sanatorium treatment for tuberculosis workers were not eligible for hospital treatment. The main professional opposition came from general practitioners but hospitals also saw the legislation as a threat as it was likely that the demand for inpatient care would increase.109 The Central Hospital Council met at St Thomas’s and protested that it had not been consulted. A special committee of the British Hospitals Association drew up a memorandum to the Chancellor of the Exchequer stating that the act would reduce subscriptions and interfere with the training of students. Mr Lloyd George received a delegation and was asked if payment could be made to the hospitals for accidents, serious or unusual diseases and for those needing operations or skilled nursing. Sydney Holland told Lloyd George that it was essential that the hospitals should not be hurt, but the chancellor did not believe that subscriptions to the hospitals would be reduced merely because employers were paying part of the cost of a general practitioner service.110 The Fabian Society established an enquiry chaired by Sidney Webb which reported that even in London the principal hospitals had long waiting lists. Non-urgent cases had to wait three months for admission. For its 8 million inhabitants London had no more than two beds per thousand, when the requirement was somewhere between two and five. Webb recommended that insurance committees should contract with voluntary hospitals to ensure efficient treatment, the cost being met by an additional parliamentary vote. He thought that the provision for tuberculosis was particularly bad. No treatment was provided in hospital for incurable cases even if insured, and none for the uninsured, even if curable.111 Burdett thought that the state, as a matter of justice, should pay for the services which were the inevitable consequence of legislation, and that the hospitals should be given assistance without losing the dignity of their independent management. The Lancet said that this view was comforting if not quite convincing. The only alternative, however, was a system of state hospitals which would prove an enormous burden, estimated by the royal commissioners at £20 million per year. Was it a proposition any politician would dare to advance?112 Forty years previously The Lancet had supported the idea of a state hospital service; now it had second thoughts. There was no consensus amongst the medical profession about the relationships which should exist between doctors and the state. An extreme right party believed that beyond securing the proper education of doctors, and providing a sanitary service to safeguard the drains and control epidemics, the state should leave the medical profession alone to carry out its beneficent work in absolute independence of all government control. These devoted individualists were prepared to die in the last ditch before they would sacrifice the smallest outpost of professional liberty. An extreme left party saw salvation in the Fabian socialist proposal of state employment for all doctors. Illness could then be treated, as Beatrice Webb had suggested, as a public nuisance to be suppressed in the interests of the community, by compulsion if necessary. Some believed that the government should take responsibility for seeing that its medical employees carried out instructions faithfully to offer or force upon each member of the community the medical services the state considered necessary to maintain physical health.113 Between these two factions there was a large central party which recognised the impracticability of the ideals of the extremists, the disorder in medical charity, and the need for an honourable partnership between the state and the medical profession, to bring the benefits of medical science to individuals and society, irrespective of wealth or social position.114 The dilemma of the voluntary system The supporters of the voluntary system were becoming increasingly aware of the strengths of the competing service. In 1866 Ernest Hart had drawn attention to the possible long term effects of rebuilding the poor law infirmaries. While the infirmaries could not match the quality of care and the contribution to teaching and research of the voluntary hospitals, the voluntaries no longer had the field to themselves. LauristonShaw*, a physician to Guy’s, thought that functions might be divided, with the infirmaries handling day-to-day illnesses, while the voluntary hospitals developed specialisms to the highest level.114 This would make professional sense, whatever system of funding might ultimately be adopted. The British Medical Journal remarked that the public were coming to understand the convenience of ‘throwing themselves upon the rates’ and were doing so increasingly. In 1886 the Metropolitan Asylums Board had treated only one fever case in ten. By 1896, with a change in legislation which allowed the admission of patients who were not paupers, it was admitting 70—80 per cent. The population was being educated in the Fabians’ municipal socialism.115 The complexity of the provision and the overlap of services for the sick had been criticised by both the majority and minority reports of the Royal Commission on the poor laws, and the two reports had this in common - that the system needed radical overhaul and that extensive changes must come. The reports had re-opened the question of a coordinated state hospital service, which was debated at the annual meetings of the British Medical Association in 1910 and 1913.116 A central hospital board to coordinate services had never been formed, and while the King’s Fund was fulfilling some of its proposed functions, it could not be regarded as a central board. It was not a representative body, as was pointed out by the Metropolitan Radical Federation. The Federation said that the working classes would have more confidence in the Fund if its council was elected, like the councils of other philanthropic bodies, by its subscribers at an annual meeting. The King’s Fund pointed out that it was administered under the Act of Parliament specially passed in 1907. The Federation replied that if the act precluded the working classes from any participation it could always be amended.117 The Charity Organisation Society also criticised the fact that the Fund was not formed upon representative lines.118 Speaking to the Hospital Officers Association, the secretary to the Metropolitan Hospital said he wished that the King’s Fund Council could be augumented by representatives of the hospitals and the other central funds. Then, if housed in fine offices, a visible sign of the public’s wish to preserve the voluntary system, it would be a bulwark against municipalisation.120 His colleague at The London Hospital also rallied to the defence of the voluntaries. ‘Whatever may be the future of the voluntary hospitals’, he said, ‘nothing can rob them of their glory for the work they have done. They got on with the work while others were discussing.’22 ‘We are indeed a very patient nation’, said Dr Christopher Addison, the former dean of Charing Cross Medical School, who had become a member of parliament. Speaking at a dinner in his honour, with Lloyd George presiding, he said that it was impossible to survey the conditions of things in the capital city without coming to the conclusion that there was great room for improvement in the organisation of services.121 Sir Henry Burdett and Dr Lauriston Shaw also believed that a coordinated hospital system was urgently needed, and that the future would bring the two types of hospital into closer cooperation. Burdett thought that the solution was nearer than many people supposed. It was predicted that London would need an additional 10,000 hospital beds as a result of the National Insurance Act, and if the voluntary hospitals were not funded adequately, the poor law infirmaries would have to be turned into state hospitals. Sir William Osler, commenting on the prospects for the voluntary system at a conference in Oxford in 1913, was brief and direct. ‘Give it up’, he said. ‘It is antiquated, out of date and it is not going to continue. Make up your minds that you must accept the principle of taking pay from patients. It answers admirably elsewhere.’12 An increasing number of hospitals began to charge patients who could afford to pay. The poor law guardians were also engaged in self-examination. At their district and national conferences they debated the future, but fortified by their faith in the principles of 1834 they saw little need for the changes which had been recommended by both the reports of the Royal Commission. Reform might be necessary, but it should be reform from within, rather than the creation of an expensive new system.123 The debates came to an end in August 1914. With the outbreak of war staff were mobilized and there were wounded needing care. The hospitals and infirmaries of London, like those throughout the country, put their wards at the disposal of the War Office and the Admiralty. The hospitals were under contract to the armed services to supply a certain number of nurses in case of sudden need, and the first batch left The London Hospital on 4 August 1914. The Middlesex designated 80 beds for casualties, St Thomas’s 200, St George’s 100, St Bartholomew’s 198 and UCH 100. The London, the biggest of the hospitals, promised 500, and had purchased extra bedsteads. On August 30, a Sunday, a request was received for the admission of 100 patients that evening, the hospital to arrange the transport from Waterloo. Mr Alfred Salmon, a board member and a director of Lyons & Company, lent dozens of the firm’s vans. Whilst the patients were being received, with the mud of Flanders still upon them, there was a further request for the admission of another 200.124 A large proportion of the resident staff and many of the consulting staff of the hospitals went on active duty. Many of those who remained were attached to territorial hospitals or base hospitals. The financial and organisational problems of the hospital system were put to one side for the time being. Lauriston E Shaw MD FRCP (1859—1923); physician to Guy’s and Dean of the Medical and Dental Schools (1893—1901). Wholehearted believer in the economic and educational value of concentrating preclinical work; was secretary of the University of London’s Concentration Committee. Excellent clinical teacher. Sympathetic to the case of the Fabian Socialists, his support for contract practice and the National Insurance Bill led him into conflict with colleagues in the British Medical Association, for which he had previously been an active worker.119 1 Webb S. The London Programme. London, Swan Sonnenschein & Co, 1891. 2 Punch’s Almanack for 1899. Punch, 6 December 1888. 3 Minutes of the medical committee of the Charity Organisation Society (1871—1895). Greater London Record Office. 4 Burdett H C. The hospital problem. The Hospital, 1890, vi, p 370. 5 The proposed enquiry into medical charities. British Medical Journal, 1889, i, pp 1006, 1411; British Medical Journal, ii, p 249. 6 British Medical Journal, 1889, ii, pp 425, 1195, 1250. 7 Parliamentary Debates (Hansard) House of Lords, 28 April 1890. 8 Rentoul R R. British Medical Journal, 1889, i, p 1425; British Medical Journal, ii, pp 47—8; and The Reform of our Voluntary Medical Charities. London, Bailliere, Tindall and Cox, 1891 9 Nightingale F. In: The register of nurses’. The Hospital, 1891, 10, pp xi, xxvi, 60. 10 Monk K H. Evidence to the select committee of the Lords, 1891, para 18895; and Liickes E C E. What will trained nurses gain by joining the British Nurses Association? London, J and A Churchill, 1889. 11 First and second reports from the select committee of the House of Lords. London, Hansard and Son 1890, HMSO 1891. 12 The Lords report on the metropolitan hospitals. British Medical Journal, 1892, ii, pp 88—9, 474—5, 1069. 13 Loch C S. The confusion in medical charities. Nineteenth Century, 1892, v 32, p 298. 14 Mouat F J. The organisation of medical relief in the metropolis. Lancet, 1893, i, pp 45, 378, 546, 812. 15 Burdett H C. ed. Hospitals and charities 1894, 5th Edition. London, The Scientific Press, 1894. 16 The Lords committee. The Hospital, 1892, 12, pp 263, 289. 17 Twining L. Charities. The Economic Review, 1895, 5, p 476. 18 The proposed central hospital board for London. British Medical Journal, 1897, ii, p 1813; Lancet, 1897, i, pp 255, 336; and Lancet, 1897, ii, pp 1612—4. 19 The minutes of the Central Hospital Council. Westminster Hospital archives H2/WH(5); and British Medical Journal, 1897, ii, p 1608. 20 Report of the committee appointed by the Hospitals Reform Association to enquire into the working of special hospitals. Lancet, 1897, i, pp 104 1—7, 1657; Hospital Reform Conference. British Medical Journal, 1897 ii, pp 1272—7; and The Hospital, 1899, 14 October 1899, pp 34—7. 21 King’s Fund A/KE/569/8. 22 Morris E W A. History of The London Hospital. London, Edward Arnold, 1910. See also Gore J. Sydney Holland: Lord Knutsford: a memoir. London, John Murray, 1936. 23 The outpatient question. British Medical Journal, 1897, ii, p 1351. 24 The Metropolitan Asylums Board. Lancet, 1886, i, pp 163, 554—5. 25 London health administration. Lancet, 1894, i, p 1456. 26 Annual report of University College Hospital 1896 and British Medical Journal, 1897, ii, p 1805. 27 Lee S. King Edward VII: a biography, vol 1. London, Macmillan and Co, 1925, pp 619—23. 28 The Queen’s commemoration fund. Lancet, 1897, i, pp 48, 192. 29 Lancet, 1897, i, pp 327, 388, 462. 30 King’s Fund A/KE/45. 31 King’s Fund A/KE/567 and /567/40(e). 32 First report of the Prince of Wales’ Hospital Fund for London. London, Prince of Wales’ Hospital Fund, 1897. 33 Lancet, 1897, i, p 1653. 34 King’s Fund A/KE/568. 35 Lancet, 1897, i, p 1220. 36 The Prince of Wales’ Hospital Fund. British Medical Journal, 1897, i, p 865. 37 King’s Fund A/KE/283. 38 The ‘Lister Letter’. A/KE/569/8. 39 A/KE/570. 40 Long F D. King Edward’s Hospital Fund for London: the story of its foundation and achievements. London, King’s Fund, 1942. 41 A/KE/281; A/KE/283. 42 Metropolitan Radical Federation Memorial. Lancet, 1900, i, p 1825. 43 Burdett H C. The medical attendance of Londoners. London, Scientific Press, 1903. 44 Report of the committee appointed to enquire into the financial relations between hospitals and medical schools in London. (Chairman: Sir Edward Fry). London, King’s Fund, 1905. 45 A/KE/281. 46 A/KE/285. 47 The Fund’s rule as to the financial relations between hospitals and medical schools. A/KE/536(3). King’s Fund, 1933. 48 Hunter W. Historical account of Charing Cross Hospital and Medical School. London, John Murray, 1913; and A/KE/571 (46) and (47). 49 Squire-Sprigge S. Medicine and the public. London, Heinemann, 1905; and Squire-Sprigge S. Medical education. London, Bailliere, Tindall and Cox, 1910. 50 Moxon W. Medical education in London. Lancet, 1886, i, pp 945—6. 51 The gift to University College and medical education. Lancet, 1904, i, pp 880—1. 52 Medicine and London University. British Medical Journal, 1908, i, p 946. 53 Medicine and London University. British Medical Journal, 1908, ii, pp 214, 1633. 54 Osler W. Functions of an outpatient department. British Medical Journal, 1908, i p 1470. 55 Osler W. The hospital unit in university work. Lancet, 1911, i, pp 211, 249. 56 Flexner A. Medical education in Europe. New York, Carnegie Foundation, 1912. 57 Final report of the Royal Commission on University Education in London (Chairman: R B Haldane) 1913. Abstracted in The Lancet, 1913, i, pp 1184—6, 1251, 1336—7, 1410—1. 58 The University of London. Lancet, 1913, i, pp 835—7; ii, pp 1482—3, 1914. 59 Newman Sir George. The building of a nation’s health. London, Macmillan, 1939. 60 Foster Sir M. Medical science and the hospitals. Nineteenth Century, 1901, 49, p 57. 61 Postgraduation study. British Medical Journal, 1908, ii, p 674. 62 Hawthorne C 0. The present position of postgraduate medical education. Lancet, 1913, ii, p 707. 63 Postgraduate study. Lancet, 1913, ii, p 745. 64 Young K E and Garside P L. Metropolitan London: policies and urban change 1837—1981. London, Edward Arnold, 1982. 65 Burdett H C. Hospitals and asylums of the world, Volumes 3 and 4 incl. Introduction. London, J and A Churchill & Scientific Press, 1893; and Beale P T B. The prospects of general hospitals. Lancet, 1902, i, pp 990—1. 66 King’s Fund A/KE/246/6. 67 Daily Mail, 15 November 1902; The Hospital, 22 November 1902, pp 133—5. 68 Daily Mail, 27 November 1902 onwards. 69 Daily Mail, 6 December 1902. 70 Unequal distribution of hospitals in the metropolis. The Hospital, 7 March 1903, pp 394—6. 71 The question of hospital sites in London. The Hospital, 10 January 1903, pp 252—5. 72 The hospital problem in London. Lancet, 1903, i, pp 676, 750—2. 73 St Bartholomew’s Hospital. Lancet, 1903, i, pp 180, 1389; Lancet, 1903, ii, pp 1587—8; Lancet, 1904, i, p 317; St Bartholomew’s Ha/6/6/1. 74 St George’s Hospital. The Times, 20 June 1904; Lancet, 1904, i, pp 743. 75 King’s Fund A/KE/570. 76 King’s Fund A/KE/259/9. 77 Sites and population in London. The Hospital, 1903, p 394. 78 King’s Fund A/KE/571 nos 48—68. 79 The amalgamation of St George’s and the Westminster Hospital. Lancet, 1913, ii, pp 157. 80 King’s Fund A/KE/279. 81 King’s Fund A/KE/570. 82 King’s Fund A/KE/278. 83 King’s Fund annual report 1906. 84 Burdett H C. Ed. Hospitals and charities, 1905. London, Scientific Press. 85 A magnificent bequest. Lancet, 1900, i, p 428. 86 The future of London hospitals. British Medical Journal, 1908, i, pp 15 13—5. 87 The apathy of Londoners with regard to their hospitals. Lancet, 1906, i, p 1185. 88 Hospital finance. British Medical Journal, 1908, i, pp 44, 1493, 1515; Hospital economics: the statistical reports of the King’s Fund. The Hospital, 1913, v, pp 55, 227, 287, 423. 89 Statistical report on the ordinary expenditure of sixteen London hospitals for 1903. London, King’s Fund, 1904. 90 Revised uniform system of hospital accounts. London, King Edward’s Hospital Fund for London, 1914. 91 Morris E W. The economical management of a voluntary hospital. London, Geo Barber, 1906. pp 43—5. 92 The Metropolitan Sunday Fund and cinema shows. Lancet, 1911, i, pp 761, 889, 911. 93 British Medical Journal, 1906, ii, pp 268, 321, 965, 1880—1 and supplement p 221. 94 UK hospitals conference. The Hospital, 15 December 1906, pp 194—200. 95 Do hospitals give excessive free relief? Hospital Officers Association. The Hospital, 29 December 1906, pp 234—6. 96 The second UK hospitals conference. British Medical Journal, 1908, i, pp 458, 886 and supplement pp 148—165; and The Hospital, 1908, 44, p 27. 97 Enquiry into the management of outpatient departments. London, King’s Fund, 1912 and A/KE/47. 98 F Lawson Dodd. A national medical service. London, Fabian Society, 1911. 99 Royal Commission on the Poor Laws and the Relief of Distress. Report. (Chairman: Lord George Hamilton). London, HMSO, 1909. Cd 4499. 100 Roberts N. The overlapping work of the voluntary general hospitals with that of poor law relief. Appendix 22. Royal Commission on the Poor Laws, 1909. 101 Burdett H C. The British Hospitals Association. The Hospital, 1910, 48, p 745. 102 Loch C S. The social policy of the voluntary hospitals. The Hospital, 1910, 49, p 83. 103 Webb B. The coming of a unified county medical service and how it will affect the voluntary hospitals. The Hospital, 1910, 49, p 139. 104 Annual report of the Local Government Board, 1899. 105 Saxon-Snell A. Infirmary v hospital architecture. The Hospital, 1913, 54, p 17—19. 106 Twining L. Evidence to the Lords Committee 1891, paras 22635 et seq; and Watkin P J. Lambeth Hospital: fifty years retrospect. London, Buck and Wooton, 1954. 107 Thackray Parsons C. The reform of poor law medical relief. In: Poor law conferences 1909—19 10. London. P 5 King, 1910; and The present and future of the poor law infirmary, Lancet, 1910, i, pp 67, 741. 108 Charity organisation and pauperism. Lancet, 1900, i, p 1024. 109 National insurance and the voluntary hospitals. Lancet, 1913, i, pp 182— 3; ii pp 319-.320 110 British Hospitals Association papers held by the London School of Economics. 111 Special supplement on the working of the National Insurance Act. (Chairman: Sidney Webb). New Statesman, 14 March 1914, II, no 49. 112 BMA conference — hospitals and the state. Lancet, 1913, ii, pp 90, 402. 113 Moore B. The dawn of the health age. London,J and A Churchill, 1911; Webb B. Our Partnership. London, Longmans Green and Co, 1948, p 348; and Sidney and Beatrice Webb. The state and the doctor. London, Longmans Green and Co, 1910. 114 Shaw, Lauriston E. The future of the voluntary hospital. British Medical Journal, 1908, p 1741; Order and charity. Lancet, 1910, ii, p 1813; Lancet, 1911, i, pp 38—9; Medicine and the state. Lancet, 1918, ii, pp 87—90. 115 The growth of the Metropolitan Asylums Board. British Medical Journal, 1897, ii, p 360. 116 The Hospital, 1913, 5 July 1913, p 423; Lancet, 1910, ii, pp 407—8. 117 The King’s Fund. The Hospital, 1910, 49, pp 265, 299. 118 Annual charities register and digest. London, Charity Organisation Society, Longmans Green and Co, 1913. 119 Lauriston E Shaw (Obituary). British Medical Journal, 1924, i, p 40. 120 Courtney Buchanan J. The function of the voluntary hospitals. London, Whitefriars Press, 1911. 121 Addison C. The health of the people. London, University of London Press, 1914; and Lancet, 1914, i, p 483. 122 Osler Sir W. The British hospital system: presidential address. The Hospital, 1913, 54, pp 411—3; Lancet, 1913, ii, p 89. 123 Report of the poor law conferences, 1910—1911. 124 Morris E W. The London Hospital (3rd Edition). London, Edward Arnold, 1926.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 A
comparable situation existed in municipal government where the
metropolis lagged behind provincial cities. The London boroughs were
not formed until 1899 and there was no single elected body which
could speak for the capital as a whole. In the absence of borough
councils most duties devolved on 29 administrative vestries, 44
non-administrative vestries, 12 district boards, 1 local board of
health, 12 burial boards, 19 boards of library commissioners, 10
boards of baths and wash-houses commissioners, the boards of
guardians and the Metropolitan Asylums Board. Since the 1860s a
campaign led by the London Municipal Reform League had urged the
case for a single central elected authority, a demand opposed by the
City of London and the vestries who sought greater municipal
dignities for themselves. After many reverses, the Local Government
Act (1888) established the London County Council and abolished the
unlamented Board of Works which had achieved the doubtful
distinction of the nickname, ‘Board of Perks’. Mr. Punch, in his
A
comparable situation existed in municipal government where the
metropolis lagged behind provincial cities. The London boroughs were
not formed until 1899 and there was no single elected body which
could speak for the capital as a whole. In the absence of borough
councils most duties devolved on 29 administrative vestries, 44
non-administrative vestries, 12 district boards, 1 local board of
health, 12 burial boards, 19 boards of library commissioners, 10
boards of baths and wash-houses commissioners, the boards of
guardians and the Metropolitan Asylums Board. Since the 1860s a
campaign led by the London Municipal Reform League had urged the
case for a single central elected authority, a demand opposed by the
City of London and the vestries who sought greater municipal
dignities for themselves. After many reverses, the Local Government
Act (1888) established the London County Council and abolished the
unlamented Board of Works which had achieved the doubtful
distinction of the nickname, ‘Board of Perks’. Mr. Punch, in his
 rt
when it was not forthcoming. Sydney Holland at one time
considered
rt
when it was not forthcoming. Sydney Holland at one time
considered