|
It is now necessary to break the continuity of the narrative, which is essentially chronological, to consider the development of two concepts which increasingly influenced the development of hospital systems in this country. They were hospital districts and regionalisation. Both can be traced back for many years and neither is specific to London. The ideas can be found in hospital and medical literature from the end of the nineteenth century, in the report of the Select Committee of the House of Lords on Metropolitan Hospitals1, and in the writings of the Fabian socialists.2 By the outbreak of war in 1939 such organisational concepts were being widely discussed, as was the role of county councils in the provision of health care. However, while the leaders of the voluntary hospital movement frequently urged hospitals to think about matters outside their walls, and to take a national view, they generally saw little need to do so. As a national hospital service became increasingly likely, the necessity became more pressing. Independence of management and local traditions were not going to persist for ever, and hospitals needed to present a united front on many issues. Districts and regionalisation were amongst the matters on which a hospital view was called for. The London services might have longstanding traditions, but the problems of the capital’s hospitals, although complex, had to be solved within a framework of wider policies. Institutional care had been provided by geographically based organisations for many years. The role of parishes in the care of the poor had been accepted since the statute of 1601, the ‘43rd Elizabeth’. There was therefore nothing new in the idea of institutions within the poor law having a district responsibility. The municipal hospitals later worked on the same basis. However, the voluntary hospitals and medical charities seldom set a boundary to their responsibilities. They might have been established to meet a pressing local need, but a residential test was not applied before deserving cases were admitted. The idea of a district hospital, providing a higher level of care than customary under the poor law, to which incurable cases of cancer, dropsy and consumption might be sent, was raised by Louisa Twining in her evidence to the Select Committee on Poor Relief in 1861.3 A parallel was drawn with the newly established district schools. At the hospital conference of 1881 Henry Burdett suggested that each large hospital should be the centre of a district, an idea later echoed by Mouat.4’5 Most plans for hospital systems produced after the conference suggested the organisation of services on a district basis. The affiliation of voluntary and rate-supported hospitals and the provident dispensaries, to provide a united district service, was proposed by witnesses to the select committee of the House of Lords in 1890, including the Charity Organisation Society. This was too radical an idea at the time for there was no general acceptance of the view that all institutions in a locality should cooperate in the provision of services. Neither was there any desire on the part of the voluntary hospitals to determine the areas for which services might be planned. A memorandum prepared in 1918 by the Labour Party’s advisory committee on public health described in some detail how a hospital service might be organised, and is remarkably modem in its approach.2 However, Sir Bertrand Dawson KCVO, physician at The London Hospital, is generally credited with the first definitive statement of the principles of organisation of a complete hospital system. Bertrand Dawson developed his ideas on system in health services while in the Royal Army Medical Corps, where organisation, adjustment and planning saved lives. As a physician to the Royal Family with an extensive private practice, he was well known and respected in political circles and involved in discussions on the future Ministry of Health. His views on the need to centralise certain specialised activities were outlined in his Cavendish Lectures to the West London Medico-Chirugical Society on "The Nation's Welfare and the Future of the Medical Profession" of 19186, on which The Lancet commented favourably.7 Dawson urged the medical profession to take a lead. Dr Christopher Addison, the first Minister of Health and former dean of the Charing Cross Hospital Medical School, was therefore well aware of his thinking when, in October 1919, he asked Dawson to chair a consultative council to advise on ‘schemes for the systematised provision of medical and allied services, as should be available, for the inhabitants of a given area. 8 Before the report was published Dawson was elevated to the peerage as Lord Dawson of Penn. Lloyd George felt there was a real advantage in having in the House of Lords some real authority on public health.
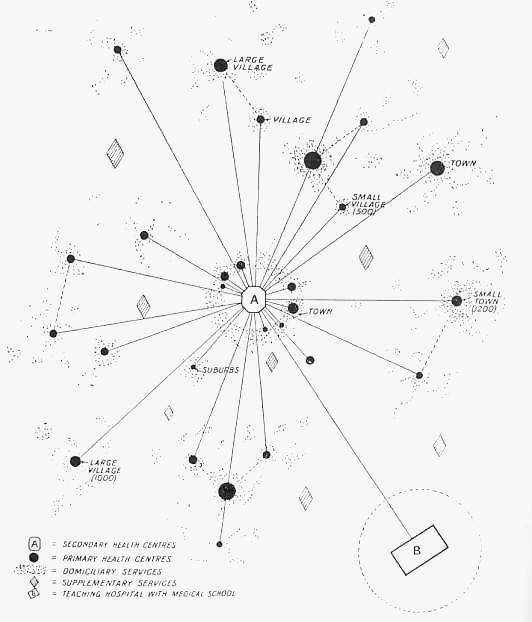
Source: Great Britain, Ministry of Health, Consultative Council on Medical and Allied Services, Interim Report. (Chairman Lord Dawson) London HMSO 1920 Cmd 693 Implicit in the report, much of
which was based on ideas Dawson himself put forward, were the concepts
of district and regionally based services. The Medical Officer of Health
for Gloucestershire, Dr J Middleton Martin, had been thinking along
similar lines, and had made co-operation a reality in his locality.
He wrote to Dawson after his Cavendish lectures about this practical
example.. The council suggested a hierarchical system which proceeded
from the simple to the complex. Domiciliary services would be supported
by primary health centres staffed by general practitioners with the help
of laboratories, radiography and inpatient accommodation. In nearby
towns, secondary health centres would provide a full range of general
and specialised medical services, with medicine, surgery, gynaecology,
ophthalmology and ENT as a minimum. These hospitals would relate in turn
to university hospitals where the rarest and most difficult cases might
be managed. The scheme would require a new pattern of medical
administration, to ensure ‘unity of purpose at all levels’. It was
proposed that there should be a single health authority to unify and
control all health services, curative and preventive, much stress being
laid upon the latter. As to the constitution of the Health Authority the
members When the report appeared the British Medical Journal commented that its implementation would have a profound effect on the future of medicine in England.9 The Hospital said it was of transcendent importance but that its proposals would be costly and its implementation would inevitably entail the disappearance of the voluntary hospital system, as then known.10 The report was inherently controversial for district organisation would only be possible if hospitals sacrificed some of their autonomy. The organisation of services to cover wide areas was a challenge to the concept of local government and its boundaries. In the event the reaction was muted, for many of the ideas had been advocated previously in one form or another, and their implementation seemed too distant to be a real threat. There had been disagreements in the consultative council about financial matters, and whether health authorities should be statutory committees of existing local authorities, or ad hoc bodies established purely to manage health services. A final report never appeared. The model scheme quickly came to pieces, and the potential cost of building and maintaining the services likely to be required was an embarrassment to the government.11 The financial crisis which developed just as the report was published delivered the coup de grace, and a document which now appears a crucial if idealistic statement of the shape a health service system should take was discounted at the time. The council ceased to meet shortly after the publication of its interim and only report. Organising hospital services on a district basis stems naturally from the needs of a population for day-to-day care. The rarer complex cases requiring more specialised care demand larger catchment populations. A regional hospital system providing specialist services had few precedents and the idea suffered from close identification with the interests of the larger voluntary hospitals, which were the main providers of specialist care. Dawson’s writings had expounded the principles of the organisation of services for large areas, and the reference of patients to distant specialist centres was slowly becoming established practice. The organisation of a hospital system to facilitate this was a new idea. The voluntary hospitals felt the need to combine in defence of their own interests, and regionalisation was an obvious and convenient method of dealing with practical problems on a geographic basis - even though it did not find many parallels in local government.12 In 1935 the British Hospitals Association, realising the seriousness of the hospitals’ financial position, established a commission under the chairmanship of Lord Sankey to consider collaboration within the voluntary movement. Its report, published in 1937, recommended the formation of regional hospital councils. While noting the ‘freedom of spirit and of action of the voluntary hospital movement’, the commission pointed out that competition between voluntary hospitals and with the growing municipal hospital service was wasteful. The regional hospital councils would be based on the organisation of the British Hospitals Association, coordinated by a central council. 13 Regional councils would have offices and staff, would coordinate hospital work, and might in time administer a regional fund so that a hospital with a surplus could help one with a deficit. The regional councils would define the functions of hospitals in their areas, ‘grade’ them, keep bed states and patient records, organise an ambulance and blood transfusion service, keep statistics, arrange the joint purchase of supplies, and publish regular reports. Lord Sankey thought that two things were necessary if his report was to be implemented: the constant thought and attention of public spirited men and women, and money. His report was widely welcomed but largely for reasons of finance the British Hospitals Association took no active steps to implement the recommendations. The scheme remained in abeyance. (see map below) Policy and Economic Planning, in its broadsheet and its Report on the British Health Services, supported regionalisation and quoted with approval the recommendation of a royal commission on local government in Tyneside, that for efficiency and economy medical services and hospitals should be administered by a single regional authority covering a wide area.15, 16
The danger of war in 1938 led to a further exercise in regionalisation. The Ministry of Health, after discussion with the local authorities and the voluntary hospitals, began to survey hospitals and infirmaries and to classify them according to the facilities they provided, linking those in vulnerable areas with others in more distant places. For the purposes of the survey the Ministry, in discussion with Mr Orde, adopted the British Hospitals Association regions.18 Medical officers were appointed to work out the details of an emergency organisation for different parts of the country, and in the south-east three hospital officers, based at the Ministry itself, were responsible for region six. When war broke out in 1939 the Emergency Medical Service came into being and a regional form of organisation was established overnight. There was a suggestion that the Government should go the whole hog and establish a centralised state hospital service from the first months of the war. Less radical counsels prevailed, but Sir Edward Forber, a retired civil servant who was considering postwar hospital policy at the Ministry of Health, suggested in November 1939 that an investigation into possible health region boundaries should be started.19 The Nuffleld Provincial Hospitals Trust In 1935 an informal grouping of voluntary and municipal hospitals in Oxford was established with the support of Lord Nuffield (1877—1963). This successful collaboration between hospital systems which elsewhere were often rivals was followed by the establishment of the Nuffield Provincial Hospitals Trust. In October 1939 Lord Nuffield wrote to the Minister of Health, Mr Walter Elliot, introducing the deputy chairman of Barclay’s Bank, Mr William Goodenough, who had a long experience of hospital affairs at the Radcliffe Infirmary in Oxford. Goodenough brought a proposal for the establishment of a trust, to which Lord Nuffield was proposing to give a million shares in Morris Motors Ltd valued at £1,250,000. Here was the money for which Lord Sankey had been hoping. On the face of it a parallel existed with King Edward’s Hospital Fund for London but it was clear from the start that the Fund and the Trust would differ in their emphasis. The Fund contributed significantly to the revenue of London’s voluntary hospitals but even as large a gift as was in prospect could have little effect on the finances of the provincial hospitals. The prime object of the new trust would be to encourage regionalisation, coordinating municipal and voluntary hospitals, and ancillary services. The Minister considered his position in relation to the new trust carefully. There had to be visible support for the voluntary principle and regionalisation was the most hopeful approach apparent, but he could not become committed to details in advance of a general government statement on hospital policy. Competition with the King’s Fund also had to be avoided, but the gift was welcomed in the House and widely publicised in the press on 6 November 1939.20 The basis of the plan developed by the Trust in the next few months was the demarcation of the country into a series of hospital regions, each having as the focus of hospital and health services a university medical school and a ‘key’ hospital. The regions were divided into hospital divisions, each with a main hospital at the core to which the smaller hospitals and clinics of the division were linked. In turn the divisional hospitals were linked to the regional key hospital. The Trust was able to build upon a number of schemes which were already being developed,12 and four regional and eleven divisional councils had been formed by the time of the announcement of the government’s post-war hospital policy in 1941. The search for coordination was always pursued as a means of ensuring that the patient might find a good and complete service in his own area, never in the interests of administrative convenience.21 The speed of the Nuffield Trust’s progress began to worry the local authorities, including the London County Council, who felt that the Trust was forcing the pace. They were not reassured by occasional remarks by leading members of the Trust about the importance of maintaining voluntarism and avoiding state shackles. It soon became apparent to the Nuffield Provincial Hospitals Trust that the natural units of hospital organisation were related to catchment patterns, and not to home defence regions or county boundaries. The Trust sought ministerial endorsement of its aims, first from Mr Malcolm Macdonald and then from Mr Ernest Brown when he took over the Ministry. Endorsement was given in guarded terms. Ministry officers were encouraged to attend regional council meetings, but only as observers who were unable to commit themselves until there had been a government announcement about post-war hospital policy. It was inevitable that the local authorities should see regionalisation as a threat not only to their own services, but to the whole concept of local government. They naturally favoured local authority control, and disliked the prospect of a regional council advising on provision over a territory wider than their own areas. In general the medical profession and the reports produced by bodies like the British Medical Association favoured the regional concept.22 The Ministry of Health was caught between the two forces. The Minister, Mr Malcolm Macdonald, wrote to the Trust in January 1941 supporting their efforts in preparing the ground for future action; he believed that the ultimate hospital service should be built upon the foundation of existing organisations and was ‘convinced that the problem was one which must be examined on a basis wider than that of existing local government areas, and that some form of regional unit will be necessary in designing a system which will make the best use of our existing hospital accommodation and will avoid duplication and waste in making good any deficiencies’. There is, however, a distinction between ‘designing’ and ‘operating’.23 Anxieties that the Nuffield Trust was likely to establish a pattern for the future before others had developed their own ideas were communicated to the Ministry. On 9 October, the day before the Trust was due to consider a memorandum on ‘A National Hospital Service’, there was a somewhat precipitate announcement of the government’s post-war hospital policy in the House. The memorandum on ‘A National Hospital Service’ brought together the Trust’s proposals.21 Stating that there was increasing recognition of the need for coordination, it was maintained that a scheme to coordinate the hospitals would produce the most effective use of resources. Were the voluntary system to be abolished, however, the substitution of state hospitals would place a considerable load on exchequer funds - the type of remark which had led the local authorities to suspect the Trust of being primarily concerned with the defence of the voluntary movement. The British Hospitals Association, which had been advocating regionalisation before the Nuffield Trust was founded, rapidly produced its own memorandum. Stressing its commitment to regionalisation since the appearance of the Sankey report, the Association said that the area of coordination ‘when circumscribed is not to be regarded as surrounded by Chinese wails or unbreakable barriers. The area is simply a unit formed after consideration of a number of factors such as the nature of the hospital services generally available, the present natural flow of patients, the nature and spheres of influence of the local authorities concerned, questions of transport and questions of geography’.22 After the Minister’s announcement of post-war hospital policy in the House on 9 October 1941, William Goodenough was asked to ‘go slow’ on the formation of regional councils.24 He had demonstrated his grasp of hospital matters and there were other jobs in store for him. The Ministry was concerned about the organisation and financing of medical education. Regionalisation had become a baffle-ground of conflicting forces. Groups like one chaired by Sir Wilson Jameson at the London School of Hygiene and Tropical Medicine, before he became the Ministry’s chief medical officer, and the Medical Planning Commission (1942)25, developed the Dawson concept of a hierarchical service. The population needed for such a structure was of the order of two million. It was a professional concept, meeting the needs of specialist medicine and consistent with the desire to associate a university and its medical school with the health authority. Indeed the proponents of regionalisation could not visualise a region without a medical school at its centre. While the administrative county of London was itself equal in size to any of the regions being discussed, the London County Council was particularly hostile to any suggestion of regionalisation. Its vision of a region was the London County Council dominating the hospital services. In the provinces, regional councils were being set up in collaboration with local authorities, but in London the LCC was unwilling to play.26 The idea of regional groupings had been in the air since the Sankey report (1937). The Nuffield Trust, backed by its money, had begun to bring it - or something like it - to earth.27 The idea of the two systems working together was unimpeachable, but whether it was practicable was another matter. As advisory bodies without executive powers, Sir Frederick Menzies doubted whether regional councils could ever be effective. He thought that ‘a paper scheme in which in which the municipal hospitals and the voluntary hospitals are to merge themselves into a Regional Council for a given area by a series of resolutions, based on mutual sacrifice of their rights and responsibilities would never work in actual practice’. He felt it was too much to expect of them. Neither hospital organisation was constituted in that way in London, even if they were in the shires. The scheme savoured of the armchair and the calm of the academic cloister. Nevertheless he believed that the King’s Fund and the London Voluntary Hospitals Committee should discuss the proposition, and he wrote to the Minister of Health, after his retirement, suggesting that if regional councils were formed, the Minister should nominate representatives to help overcome the mutual suspicion and distrust. Menzies had a practical touch; the altruistic cooperation of reasonable men was an inadequate foundation for regionalisation.28 When regions came, they were more solidly based. Indeed, the entire structure of the health service was established upon a regional basis, with a lower tier providing services for health districts.
1 Report on the metropolitan hospitals from the select committee of the House of Lords. Indexed under ‘Territorial and affiliation system for hospitals’. London, HMSO, 1892. 2 The organisation of preventative and curative medical services. London, Labour Party, 1918; and The Medical Officer, 1920, pp 113—115. 3 Twining L. Evidence to the select committee on poor relief, paras 11619 and seq, 11965 and seq. 4 Burdett H C. Address to the hospital conference, reprinted as Hospitals and the state. London, J and A Churchill, 1881. 5 Mouat F. The organisation of medical relief in the metropolis. Lancet, 1893, i, pp 45, 378, 546, 812.
6
Dawson Sir Bertrand. The future of the medical profession. (Cavendish
Lecture). Lancet, 1918, ii, pp 83—5. and see 7 Medicine, parliament and public. Lancet, 1919, i, p 267. 8 Great Britain, Ministry of Health, Consultative Council on Medical and Allied Services. Interim report on the future provision of medical and allied services. (Chairman: Lord Dawson). London, HMSO, 1920. Cmd 693; Dawson Lord. Medicine and the State. The Medical Officer, 1920, pp 223—4; PRO/MH/73/49; see also Honigsbaum F. The division in British medicine. London, Kogan Page, 1978.
9
The report of the consultative council. British Medical Journal, 1920,
i, Editorial p 746-7, summary of the report pp 737-743 10 Lord Dawson’s scheme. The Hospital, 1920, pp 239, 345—6. 11 PRO/MH/73/3 1. Minutes of the consultative council on general health questions, 10 December 1920. (Dr Addison’s comments). 12 Hospitals year book 1940. London, Central Bureau of Hospital Information, 1940. 13 Report of the Voluntary Hospitals Commission. (Chairman: Lord Sankey). London, British Hospitals Association, 1937. 14 King’s Fund A/KE/224. Lancet, 1937, i, pp 1123, 1352; 1937, ii, pp 1156—7. 15 The hospital system. London, Political and Economic Planning, iv, no 84. 16 Report on the British health services. London, Political and Economic Planning, 1937. 17 Orde R P. Regionalisation. An essay in the Hospitals year book 1939. London, British Hospitals Association, 1939. 18 PRO/MH/55/624. 19 PRO/MH/80/24. 20 PRO/MH/58/324—326; A central hospital fund. Lancet, 1939, ii, p 1272. 21 A national hospital service — a memorandum on the co-ordination of hospital services. Nuffield Provincial Hospitals Trust, 1941. 22 The regionalisation of hospital services. London, British Hospitals Association, 1941. 23 PRO/MH/58/326. 24 PRO/MH/77/1. 25 Medical Planning Commission. Draft interim report. London, British Medical Association, 1942. 26 King’s Fund A/KE/224. 27 PRO/MH/80/24. (This file contains extensive material on regionalisation.) 28 King’s Fund A/KE/95.
|